
Abstract
Social robots are increasingly used in the care of older adults, including people living with dementia. An important prerequisite for effective use is knowledge about which factors facilitate and hinder the acceptance of social robots. The aim of this review at the intersection of health care research and human–robot interaction research is to understand factors facilitating and hindering the acceptance of social robots for older adults and people living with dementia in nursing homes based on the Almere model and to identify research gaps. We conducted a scoping review, systematically searching MEDLINE, PsycINFO, CINAHL and Compendex. The Almere model of acceptance was used to guide the development and conduct of this review. We used the principles of deductive content analysis, and we narratively present the review results. Twenty-six studies were included in the review. We found facilitating and/or hindering factors for all constructs of the Almere model. Perceived usefulness, perceived ease of use and perceived enjoyment were the most studied constructs, whereas trust and intention to use were the least studied constructs. Across constructs, seeing robots positively impacting residents was one of the key facilitating factors, and practical difficulties were a hindering factor. The Almere model provided useful insight into the acceptance of social robots. Nevertheless, we found the concept of engagement, the nursing home context, the intervention characteristics and the individual user groups important for the acceptance of social robots in nursing homes and therefore argue for future research expanding on the model.
Similar content being viewed by others


1 Introduction
The number of older adults over the age of 60 is increasing globally, and this trend is accelerating. In 2019, there were 1 billion older adults, and according to the World Health Organization (WHO), this number will rise to 1.4 billion by 2030 and 2.1 billion by 2050 [1]. Dementia is one of the primary causes of disability and dependency among older adults globally. Worldwide, approximately 50 million people have dementia, and this number is estimated to rise to 80 million people in 2030 and 152 million in 2050 [2]. When care needs increase and caring for people living with dementia (PlwD) is no longer possible in their own homes, PlwD often move to a nursing home. However, it is estimated that the nursing home capacity is not rising in accordance with the growth in the number of PlwD. It is therefore a challenge to provide high-quality care in nursing homes [3]. One strategy to improve the care of PlwD and older adults is the use of social robots. Social robots are currently being developed, tested and implemented in nursing homes to improve care for older adults and PlwD in the future. Social robots are a subtype of robots and robotic devices, as illustrated in Fig. 1; for social robots, the primary focus is not on productivity or efficiency, as is often the case with industrial robots, but on social interactions and companionships [4].

Shows the categorization of robots [4, p. 13]
In this review, we apply the following definition of social robots from Naneva et al. “We define a social robot as a physically embodied artificial agent (i.e., something that has a physical structure that mimics the behaviour, appearance, or movement of a living being—usually a human, but could also be an animal or plant) that: (a) has features that enable humans to perceive the agent as a social entity (e.g., eyes); (b) is capable of interacting with humans via a social interface; and (c) can communicate verbal and/or non-verbal information to humans” [5]. Social robots come in many shapes and sizes. They are typically either zoomorphic (i.e., pet robots such as the robot seal Paro [7], the robot cat NeCoRo [8] and the robot dog Sony Aibo [9] or humanoid, such as the robots Mario [10,11,12], Silbot [13, 14], Telenoid [15, 16] and Pepper [17, 18]. However, social robots can also be telepresence robots, such as Giraff [19], that facilitate interactions between a resident and his or her family members by facilitating video calls on a tablet attached to a mobile, remotely controlled robot. Some social robots were designed specifically for dementia care (e.g., Paro), while others, such as Pepper and Telenoid, were designed with completely different aims for marketing/entertainment or telecommunication but were subsequently implemented in different care contexts [7, 15, 20]. Frennert and Östlund [21] divide social robots for older adults into two research paradigms: The first paradigm positions the human users as caretakers of robots. Here, we find zoomorphic robots or robots looking like babies with the goals of companionship and cuddling. The second paradigm positions the robots as caretakers of the human users, a position that requires that the robot is to some extent able to understand the needs of a person and respond to them in social interactions [21]. Here, we have humanoid robots such as Pepper, which is able to recognize basic human emotions and react to them [22].
Previous reviews of the use of social robots in care for older adults have had a focus on mapping the use of social robots as well as looking at effect and effectiveness. These reviews concluded that there is emerging evidence that social robots are useful for engaging people in interactions, that they can have calming effects, that they can contribute to a sense of companionship, motivation and enjoyment, and that they have the potential to assist and enrich the work of nurses in several settings [23,24,25,26,27,28,29]. Studies have also shown that older adults are more likely to engage with a humanoid or zoomorphic robot than with a screen [24]. Social robots are already being used in nursing homes, and researchers expect this use to increase; however, they also argue that there is a long way to go before social robots can interact seamlessly with humans and easily become part of social life [14, 21, 24]. Previous studies have shown that the use of social robots can be demanding for staff, as robots do not independently interact with older adults but rather need assistance, explanations and prompting [14, 15, 30] and that the high cost and lack of compelling arguments for the use of social robots in health care hinder their deployment [31]. Furthermore, there are many challenges related to using robots outside of laboratories, such as oversensitive sensors and voice issues (synthetic robot voices can be hard to hear for older adults), which also demand that staff understand the related difficulties and adapt the environment to the requirements of the robot [14, 15]. Another important aspect pointed out by HRI researchers is the security level of the social robots and the risks of robots getting hacked [22, 31]. Therefore, even though there is emerging evidence on the positive effects of social robots, there are many challenges related to the use of social robots outside of laboratories as well as the acceptance of social robots in nursing homes.
Previous reviews on the acceptability and implementation of social robots among older adults have examined social robots across different settings (e.g., laboratories, private homes, nursing homes). Papadopoulos et al. found that enjoyment, usability, personalization and familiarization were enablers of the implementation of humanoid robots, whereas technical problems, limited capabilities and negative preconceptions were barriers to implementation [30]. Koh et al. found more barriers than facilitators [32]. Specifically, on the topic of intervention characteristics, many barriers, such as technical challenges and difficulties due to the complexity of the robots, were reported, whereas Koh et al. found mostly facilitators related to patients’ needs and resources, such as robots providing companionship and emotional support [32]. Both Koh and Papadopoulos concluded that there are gaps in the research on social robots related to organizations, the environment, the sociocultural milieu, policy and legal frameworks [30, 32]. In their review, Whelan et al. found that the acceptability of social robots is influenced by factors on an individual user level, as well as by the robot itself, by significant others and by social and environmental factors [33]. With regard to research designs, the authors concluded that most studies were of short duration, had small sample sizes, and did not involve actual usage of the robots in real world contexts [33]. Koh et al. further argued that the needs of PlwD living in the community and those in care settings differed but that there is a lack of literature on how social robots can be implemented in care organizations such as nursing homes [32]. In this review, we have looked into what has been published on the acceptance of social robots in nursing homes, looking at the literature, which Whelan et al. call for, when they address the need for more research on actual robot use as well as larger sample sizes, together with Koh et al.’s call for more research on the implementation of social robots in care institutions. This review addresses a gap in the literature by focusing on the specific setting of nursing homes as well as only including studies, where there were actual robot interactions and therefore looking at acceptance and not acceptability.
Defining the term nursing home internationally can be challenging, as different countries have different systems and structures of care and use different terms for similar forms of long-term residential care. In this review, we have used Sanford et al.’s internationally consensual definition of a nursing home: “A nursing home is a facility with a domestic-styled environment that provides 24-h functional support and care for persons who require assistance with ADLs [activities of daily living] and who often have complex health needs and increased vulnerability (…) In general, most nursing homes also provide some degree of support from health professionals” [34 p183-4].
1.1 Conceptual Model
Acceptance and acceptability are some of the most frequently used terms and most frequently studied phenomena in regard to social robots for older adults and PlwD [25, 32]. The terms acceptance and acceptability are often used interchangeably in the literature, but while acceptability is related to the intention to use before actual use, acceptance refers to the evaluation after the social robot has been used in practice [35]. We have chosen to use the concept of acceptance, as we want to understand how different actors evaluate a social robot after they have interacted with it in the nursing home setting.
There are multiple widely used technology acceptance models in the literature. The technology acceptance model (TAM) [36] was among the first such models; the assumption behind the model is that perceived ease of use and perceived usefulness influence attitudes towards use, which ultimately influence use. Later versions of the model (TAM2, TAM3) also consider perceived enjoyment and computer anxiety as influencing factors [35,36,37,38]. Following these developments, the unified theory of acceptance and use of technology (UTAUT) was introduced, which also includes performance, effort expectancies, social influence and facilitating conditions [38]. A later version (UTAUT2) added hedonic motivation, price value and habit with a focus on consumer behaviour [38, 39]. Other models include the Senior Technology Acceptance Model (STAM) proposed by Chen and Chan, which is based on the UTAUT and includes gerontechnology self-efficacy, gerontechnology anxiety, perceived usefulness, usage behaviour, perceived ease of use, attitude towards use and facilitating conditions [40]. Khaksar et al. build a conceptual model based on the theory of diffusion of innovation (DIT) and the TAM, adding the concepts compatibility, trialability, observability and work-related threats to the TAM [41].
Social robots differ from other technologies, as they are embodied social actors that socially interact with humans. These general technology acceptance models do not capture all the factors influencing the acceptance of social robots [4]. Heerink et al. [42] instead introduced the Almere model specifically for assessing the use of social robots for older adults, and we have used this model to guide and structure our scoping review while also including acceptance literature in the review, which does not rely on the Almere model. In this model, the authors added constructsFootnote 1 related to social interaction and older adults, specifically perceived sociability, social presence, perceived adaptivity and trust, to the variables found in previous technology acceptance models. The Almere model aims to understand both functional acceptance (ease of use, usefulness) and social acceptance (acceptance of the robot as a conversational/interaction partner). We chose this model, as it has a specific focus on social robots and includes a more comprehensive list of constructs than other acceptance models.
The Almere model was developed in 2010, and other acceptance models have been developed in the meantime. Examples include UTAUT2, STAM, the conceptual model by Khaksar et al., and the Persuasive Robots Acceptance Model (PRAM), which was based on TAM [38,39,40]. The PRAM includes perceived enjoyment from TAM3 and includes reactance, beliefs, compliance and liking. This model is specifically focused on robots that can support attitude and behaviour change and therefore includes different measures of social responses [38]. Another model is the robot acceptance model for care (RAM-care) that was developed by Turja et al. in 2020, which builds on the Almere model. They argue that the context of healthcare differs from other professional contexts and therefore needs a specific acceptance model, which includes instrumental, interpersonal and ethical values. Turja et al. add two constructs, personal values and perceived technology unemployment, and only use the constructs of the Almere model that are direct determinants of intention to use to prevent complexity in case their sample was too small for a generalized multivariate structural equation model [43]. This expanded model encompasses healthcare settings, which is directly relevant to the objective of this review. However, it omits several constructs from the original Almere model.
For the purpose of this review, we decided that the Almere model is the most comprehensive and useful acceptance model. Moreover, the model has been developed and tested specifically for older adults and social robots. Since the purpose of our study was to identify the breadth of evidence, the various constructs of the Almere model were chosen to support the comprehensive exploration of relevant constructs in this field.
In Table 1, we define the constructs of the Almere model, including moderating factors, based on Heerink et al.’s definitions. Moderating factors include age, gender, voluntariness and computer experience, which can impact the acceptance of social robots. They are not a part of the Almere model, but as Heerink et al. described, adding moderating factors to the model “(…) could complete our developed vision on the acceptance of assistive social robots and screen agents” [42, p364].
The aim of our scoping review is to provide a broad overview of facilitating and hindering factors related to the acceptance of social robots in nursing homes based on the Almere model. Furthermore, we want to understand which factors and aspects of acceptance have not been researched and to map research gaps accordingly. To the best of our knowledge, this review will be the first review to examine the acceptance of social robots specifically in the context of nursing homes. The results will guide future research at the intersection of health care research and human–robot interaction research, specifically qualitative studies, aiming to understand how social robots are experienced by end users and how they become embedded in nursing homes.
2 Methods and Analyses
2.1 Design
We chose the scoping method for this review because social robots are a relatively new technology, and research in this area at the intersection of health care research and human–robot interaction research, although increasing, is still limited. We aimed for a broad understanding of the research on the topic, and our research question therefore calls for a review that is open to different study designs. The review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews PRISMA-SCR [44] and follows the five stages identified by Arksey and O’Malley [45] as well as the advancements of the methodology proposed by Levac et al., Peters et al. and the JBI manual for evidence synthesis on scoping reviews [46,47,48].
2.2 Review Protocol
A review protocol was drafted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses Protocols (PRISMA-P) and was registered with the Open Science Framework (https://osf.io/6zxfp).
2.3 Stage 1: Identifying the Research Question
Based on the Almere model of acceptance, which shows which factors may influence the acceptance of social robots in nursing homes, this scoping review sought to answer the following question:
Which factors can facilitate and hinder the acceptance of social robots in nursing homes?
2.4 Stage 2: Identifying Relevant Studies
We used the PCC framework, which stands for P = participants, C = concept, and C = context, to identify relevant studies [48].
2.4.1 Participants
We included studies with a study population of actors in nursing homes and focused on three groups of participants: nursing home residents over the age of 60 with and without a dementia diagnosis; nursing home staff, including management; and family caregivers of nursing home residents. The age limit corresponds with the definition of the UN and WHO, who define older adults as people over the age of 60 [1, 49]. Throughout this review article, we highlight dementia. We have chosen to do this because dementia is very prevalent in nursing homes, where more than 80% of residents have dementia in most countries [34]. Symptoms of dementia diseases include disorientation, memory loss, and problems with practical activities, thinking and mood [50] and have an impact on how residents are able to interact with and evaluate a social robot. In research, there has been a tendency to exclude people with dementia, partly due to methodological and ethical challenges in including this group of people in the nursing home, who cannot always give informed consent [51, 52]. We therefore find it important to highlight this group, which makes up the majority of the residents in nursing homes. That being said, we also do look at other health conditions such as hearing impairments or problems with mobility in the results of this review, when the articles reported these as relevant for acceptance.
2.4.2 Concept
In this review, we examined assistive social robots that communicate and/or interact socially with their users. Some of these are purely companion robots, while others are also able to carry out service tasks. We chose to use the search term social robot—along with a range of other terms used to describe social robots—as other types of robots were outside the scope of this review. In the review, we included humanoid, zoomorphic or telepresence robots and excluded virtual agents, which is in line with the robot definitions of Naneva et al. and Duffy [5, 6].
The constructs found in the Almere model defined our search strategy and search string and guided our data extraction and synthesis of the results, but we also included studies that did not use the Almere model of acceptance but reported on acceptance or some of the constructs of the model. The constructs are defined in Table 1.
2.4.3 Context
We focused specifically on nursing homes, as there are large differences between social robots used in laboratory or controlled settings in comparison to actual use in nursing homes. In the lab, contextual factors are controlled, but in a nursing home, unexpected events may occur, and external influences such as background noise and background light cannot be controlled. Furthermore, nursing homes differ from private homes and other care settings, as nursing homes are simultaneously a workplace, a home and an institution with specific rules, regulations and workflows. Other care settings, such as hospital or day care, are not considered homes but are rather workplaces, whereas for home care, the setting of the care is primarily a home and not a workplace. However, nursing homes are equally homes and workplaces, resulting in different needs and regulations when implementing technology. They are also marked by three different categories of persons: Residents, staff and family, with very different affiliations with the nursing homes as well as very different needs.
As described by Sanford et al., nursing homes are defined by residents who need assistance with activities of daily living, are often vulnerable, often have complex health needs, and a majority of the residents have dementia [34]. This sets nursing home residents apart from the older adults using social robots in other settings and makes them a specific type of users of social robots. We have used the definition from Sanford et al. to screen the studies, and when we were unsure, we have looked into country-specific terms and definitions to evaluate if the care setting fell under our definition of nursing home.
2.4.4 Search
Following the PRESS 2015 guideline [53], we developed a search string for searching electronic databases that was tested, discussed and adapted continuously before finalizing the search string. The final search string for MEDLINE (via PubMed) can be found in Online Resource 1. The search strategy was based on the terms social robot and nursing home and the acceptance terms from the Almere model. We chose to use the acceptance terms from the Almere model, as the model provides a comprehensive set of acceptance terms of relevance to the use of social robots with older adults. By using the Boolean operator OR between ‘acceptance’ and the constructs of the model, this allowed us to perform a broad search of the studies on acceptance beyond simply searching for the word acceptance and its synonyms. We included literature on acceptance, regardless of their affiliation with the model. We adapted the search string to the specific demands of the individual databases and searched the titles, abstracts and keywords. We used different MeSH terms or subject headings depending on the database.
We searched MEDLINE via PubMed and PsycINFO via OVID and CINAHL via EBSCO. We filtered the results as follows: language: English; time: 2005–2020; type of source: journal article. We chose the 2005–2020 time interval because the reported research on social robots in nursing homes before 2005 is very limited. We performed the search in August 2020 and later performed an update searching of articles from 2020 until July 2022. In the search update, we additionally searched Compendex via Engineering Village. Both the original search and the search update were supplemented by hand searching and snow balling to search for additional articles.
2.5 Stage 3: Study Selection
The results from the database were imported to EndNote X9 reference management software, where duplicates were removed [54]. Thereafter, the results were imported into the review management software Covidence [55]. The screening process was a two-step process with title and abstract screening, followed by full-text screening. Both screenings were carried out independently by two reviewers (WK and SF) who both screened all papers according to the inclusion and exclusion criteria using Covidence. To increase consistency between reviewers, WK and SF discussed and tested the inclusion and exclusion criteria at the beginning of the screening process. We performed a pilot test on five papers to ensure a consistent use of the criteria before continuing with the rest of the papers. The pilot test showed that some minor adjustments and clarifications were needed, which were done before screening the remaining papers.
After the independent screening, conflicts between the two reviewers were resolved in a review meeting. When a consensus could not be reached, the other coauthors (MR, ST, BB, FL) were involved. We used this procedure for both the title abstract screening and the full text screening. The inclusion and exclusion criteria were based on the PCC framework described above, and they can be found in Online Resource 2. We included peer-reviewed published articles, specifically reviews and empirical studies. We chose not to include grey literature, as searching this literature can be a time-consuming and inefficient task leading to few results.
2.6 Stage 4: Charting the Data
Stages 4 and 5 were performed using the principles of deductive content analysis and were thus divided into three main phases: preparation, organizing and reporting [56]. In the preparation phase, we defined the search strategy and inclusion/exclusion criteria as described above and performed the search. In the organizing phase, SF, WK, ST and MR developed a structured analysis matrix based on the Almere model of acceptance and its constructs and additional categories of study characteristics, and WK and SF coded the data accordingly. Additionally, an “other themes” category was added to allow for new codes. Finally, in the reporting phase, we collated, summarized and reported the results as described in stage 5 [56].
The included articles were imported to MAXQDA 2022 [57], where metadata such as author, year and title were automatically coded. In MAXQDA, we also created a code tree with two branches (the different codes and their definitions can also be found in our codebook in Online Resource 5):
-
Study characteristics, with the subcodes: aim of study, study design, methods, study location (setting and country), participants, type of robot, duration of robot interaction, robot facilitation and outcome and instruments.
-
Acceptance
-
Acceptance (results), with the subcodes perceived adaptivity, anxiety, social presence, perceived sociability, attitude, perceived usefulness, perceived ease of use, perceived enjoyment, trust, intention to use, social influence, facilitating conditions, use, moderating factors
-
Acceptance (discussion), with the subcodes perceived adaptivity, anxiety, social presence, perceived sociability, attitude, perceived usefulness, perceived ease of use, perceived enjoyment, trust, intention to use, social influence, facilitating conditions, use, moderating factors
-
Other themes, which were used for interesting findings and themes of relevance to acceptance that did not fit into the other codes.
-
The qualitative data charting was performed independently by the two reviewers (WK and SF), who both used MAXQDA to manually code all included articles. In MAXQDA, we included definitions of the acceptance constructs from Heerink et al.’s 2010 paper [42], as well as from the UTAUT [58] (which lay the grounds for parts the model) attached as memos, so that the reviewers had the codes available during coding (see Online Resource 5 for codebook). We based the coding on the results sections of the papers to ensure that these findings on acceptance came from the article we included. To avoid losing other important insights on acceptance, we also had a set of the same acceptance codes for the discussion parts of the paper, which we have used to contextualize or discuss, when relevant. The coding was not directly related to the aims and outcome measures of the individual article; rather, we went through the results, and when we found results of relevance to a construct, for example, on ease of use, we coded that part of the text as ease of use.
We performed a pilot test to refine the data charting form and ensure that we agreed on how to use it: WK and SF discussed the definitions, individually coded three articles and then had another discussion on the codes, solving disagreements in cooperation with the other coauthors. There were some differences in the coding of the acceptance constructs, so after the pilot test, we went through all the constructs of the Almere model again to ensure that we applied them in the same way. Throughout the data charting process, conflicts were resolved between the two reviewers through discussion, and the other coauthors (MR, ST, BB, FL) were involved when a consensus between the reviewers could not be reached or we had doubts about the decision.
It was not always clear how to code the data, and differences between, e.g., social presence and perceived sociability, could sometimes be subtle—here we have drawn on the group of co-authors and repeatedly discussed to ensure appropriate coding. When writing the article, we have also sometimes returned to the coding in MAXQDA in cases where we doubted if the coding was suitable. Here, all co-authors have discussed whether changes should be made, and in a few cases, we have reassigned the codes when there was consensus on this. When needed, we contacted the authors of the articles or consulted other articles on the same study for missing information. To enhance the transparency of our coding, we have provided an example of how we coded a section of text in Online Resources 6.
2.7 Stage 5: Collating, Summarizing and Reporting the Results
The data charted in MAXQDA are presented in tabular form and narratively summarized. The data on study characteristics are presented in tabular form and narratively summarized. The data on acceptance have been summarized narratively for each of the acceptance constructs. We also visualized these results in a table. Finally, we discuss the results.
3 Results
In the results section, we present the review results, beginning with our search results. We continue by presenting the extracted data on study characteristics and on each of the constructs from the Almere model of acceptance.
3.1 Search Results
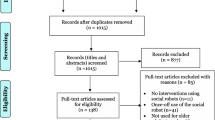
The initial database search performed in August 2020 yielded 244 results. Moreover, 35 additional records were identified by mining the references of 10 reviews found in the initial search [23, 29, 30, 59,60,61,62,63,64,65]. The 1st search update (June 2021) yielded 85 results. Additionally, 27 additional records were identified by mining the references of five reviews found in the search update [66,67,68,69,70]. The 2nd search update (July 2022) yielded 202 results; in addition to updating the previous searches, we included an additional database (Compendex) in this search. Moreover, 5 additional records were identified by mining the references of two reviews [71, 72]. After the removal of duplicates, there were a total of 388 articles for title/abstract screening, which led to the inclusion of 81 articles for full text screening. We included 26 articles in the review (Fig. 2).

PRISMA Flow Chart
3.2 Study Characteristics
The study characteristics—as well as which of the acceptance constructs from the Almere model the included studies provided results on—are summarized in Table 2. In 3.3. we go through these acceptance constructs one by one. Together they provide an overview of which papers provided results on (a) which acceptance constructs and (b) how much the different constructs were studied both from the point of view of each study and from each construct.
The 26 included articles were published between 2013 and 2022 in 20 different journals. The social robots studied were either humanoid (13 articles on eight different robots), zoomorphic (11 articles on 10 different robots) or telepresence robots (three articles on three different robots). The articles studied 21 different social robots, with the most discussed robot being Paro (n = 8), followed by Matilda (n = 4), Mario (n = 2), Pepper (n = 2), LiveNature (n = 2) and Guide, JustoCat, Kabochan, Tangy, HIRO, TIAGo, Miro, Pleo rb, Joy for All dog, Joy for All cat, Furby, Perfect Petzzz dog, GIRAFF, Double and a telepresence robot (each n = 1). Robot interaction was facilitated by staff in six studies, facilitated by researchers in five studies, unfacilitated in six studies, mixed in two studies and unclear in seven studies. The duration of robot interaction varied greatly between a single interaction and 5 years of use.
The robots were primarily tested in Europe (n = 12) and Australia (n = 9), followed by New Zealand, Canada, Hong Kong, Japan and Taiwan (each n = 1). The majority of studies (n = 16) focused on residents living with dementia. The remaining ten studies did not focus on residents living with dementia but looked at residents and carers in nursing homes and thus generally also included a large proportion of PlwD. Twenty-two of the included studies involved residents as research participants, 15 involved staff (including managers) and six involved relatives.
Regarding the study design and methods, eight of the studies applied quantitative methods, eight applied qualitative methods, and ten applied mixed methods. Sixteen studies used observations as a method, making this the most frequently used method in studies included in this review. The sample sizes differed greatly and ranged between 3 and 415 participants. Twelve of the studies took place in only one nursing home.
The aims and outcome measures of the included articles were highly diverse. In more general terms, the aims focused on investigating the experiences of carers, residents and sometimes relatives as well as evaluating the acceptance, acceptability and usability of the robots as well as engagement and interaction with the robot. The outcome measures also focused on the experiences of staff and sometimes relatives and observations of the behavioural reactions of residents to the robots. Acceptance and acceptability were often used as outcome measures.
3.3 Acceptance
To understand the relevance of each construct of the Almere model for the research field, we mapped out how many articles reported results on each construct, colour coded the constructs according to four categories and mapped the colour coding onto the model. Red means a construct was rarely studied (2–3 articles reported on it), yellow means a construct was occasionally studied (7–10 articles reported on it), orange means a construct was frequently studied (11–15 articles reported on it) and green means a construct was very frequently studied (17–18 articles reported on it) in the included articles (Fig. 3).

The Almere model coloured to reflect the review (adapted from Heerink et al. [42])
All the green constructs are direct determinants of intention to use and are simultaneously affected by other constructs of the Almere model; attitude stands out here, as it is less studied than the other constructs in this row of the model. The remaining constructs are either yellow, orange or red. Here, the red constructs trust and intention to use stand out as areas that have rarely been studied.
To summarize the data on acceptance, we present the results from our deductive content analysis on each of the constructs of the Almere model in the following. In regards to acceptance in general, eight studies reported an overall good acceptance of the robots [10, 19, 73, 76, 83, 85, 93, 94].
3.3.1 Perceived Adaptivity
Seven of the included articles provided results on adaptivity. The articles discussed adaptivity as a facilitating factor, as personalization of the activities offered by the robot as well as the ability to adapt to the various needs, abilities, sensory impairments and medical conditions of the residents were presented as factors that were important and useful and that increased the positive engagement of residents [75, 76, 83, 84, 86, 91, 94]. In one study, staff worried whether robots would be cost effective if they were personalized but found individual covers that were also washable a good way of personalizing the robots [76]. The articles here show how different kinds of adaptivity are important and related to other constructs: the ability of the robot to adapt technically to the abilities and impairments of the residents as well as the ability of the robot to adapt to what residents like, which influences both perceived usefulness and perceived enjoyment of the robot.
3.3.2 Anxiety
Eleven of the included articles had results on anxiety [19, 41, 74, 75, 81,82,83,84, 89, 90, 92]. Some reported anxiety as a hindering factor, feeling intimidated by the robot as members of staff worried about being surveyed by the robot [41, 74], were scared of the abilities of the robot and staff becoming overdependent on the robot [41] or not being in control of the robot and therefore unable to ensure the privacy of the resident [89], found the robot frightening [90] or felt insecurity and fear about making mistakes when handling the robot [75]. Some staff members also worried if residents would be afraid of the robot [19, 90].
Hindering factors for residents were the noise of Paro, which could be distressing for PlwD as well as staff [92], anxiety related to not understanding questions posed by the robot Matilda [84] and the risk that some PlwD could come to care too much about JustoCat, leading to worries [81]. Ke et al. found no change in technology anxiety after residents with dementia used a humanoid robot [82], whereas others found that most anxiety was related to the first meeting or even before meeting with the social robot and that most PlwD were not worried about the presence of the robot [19, 83, 84].
The results on anxiety show that there is a large difference in the anxieties of the staff and the anxieties of the residents. Staff worried about the robot taking over and not being in control as well as making mistakes or worried about the residents’ reactions to the robot. However, the anxiety of the residents was more related to not understanding the robot or caring too much about the robot. There is something paradoxical in this, as it seems that too much acceptance of the robot as a social actor can lead to anxiety and worries if the residents become too fond of the robotic pets.
3.3.3 Social Presence
Fourteen of the included articles had results on social presence. Residents interacting with social robots personified the robot to different degrees, with some residents thinking that the robots were real animals or that the robot was felt as a companion with a soul or as being able to see into the resident’s soul. Six articles reported this as a facilitating factor that could improve engagement and reduce loneliness and social isolation among residents [74, 75, 77, 81, 87, 91]. One article reported that staff personified the robot without evaluating it as facilitating or hindering [11], and one article reported how some staff saw the robot as cold and impersonal [90]. Five articles specifically mentioned the looks of the robots as important: Residents appreciated the colour, size and eyes of Mario [10, 11], the face and size of Matilda [84], found the eyes and faces of robots most important when comparing different types of robots [76] and felt encouraged to interact with Paro because of its appearance [91]. Here, the appearance of the robots was important for the robots to be seen as social actors—especially in regard to the face, including the eyes. In one study comparing zoomorphic robots, residents, staff and family members preferred robots designed as familiar, domestic animals, with soft furry covers and appealing face and eyes, size and weight; other robots were seen as toy-like and infantilizing [76]. Interactivity, sounds and movements were also important for the social presence of the robots, which could be facilitating [76, 93] or a hindering factor if residents wanted the robot to be able to do more, such as walking or chatting [77]. Telepresence robots were reported to increase the sense of the family being present, increasing connection and reducing social isolation [19, 89].
3.3.4 Perceived Sociability
Thirteen of the included articles had results on perceived sociability. Three articles discussed the social engagement between residents and robots [10, 78, 84]. However, whereas two reported that robots increased the social engagement of residents by making people smile, laugh, talk and interact with the robots [78, 84], the other reported that the residents did not usually verbally interact with the robot Mario and some had difficulties communicating with it [10]. Two articles reported that the robot worked as an opening to communication, which was described as an advantage facilitating its use [81, 90], whereas another article reported differential results, as residents interacted and communicated with Paro more than with Guide [92]. Three articles reported positively on using the robots for group activities helping to reduce boredom and making residents view the robots more positively [77, 84, 94]. Five articles reported that residents developed emotional bonds and companionship with robots or wanted robots to be their friends, which facilitated interactions with robots and could help residents cope with loneliness or isolation [74, 77, 83, 90, 91]. Two articles reported how residents engaged with robots as biological beings by cuddling, kissing, petting, squeezing and singing to the robots [76, 93]. Different behaviours were reported as important for improving sociability, such as pet robots having command responses (e.g., giving a paw) and demonstrating a happy mood [76], movements and sounds of Paro [77] and Matilda mixing gestures, expressions, talking, dance and music [84].
3.3.5 Attitude
Fifteen of the included articles had results on this construct. The articles reported a range of attitudes from both staff and residents, and attitude was both a facilitating and a hindering factor. Two articles found a wide range of reactions in residents from dismissal to excitement [74, 75], and one of them found that those with reactions in between could be convinced of interacting with the robots with encouragement [74]. In regard to attitude as a hindering factor, some residents were negative towards and rejected Paro [73], a minority were cautious or indifferent towards Mario, some PlwD because they felt that they would not be able to use the robot [11] and some residents were critical towards using Pepper wondering why the robots were needed and resources were spent on it [75]. Some staff were negative towards the robot, as they questioned if it was compatible with dignified care and nursing homes [75, 90], saw it as infantilizing to residents, thought it was a waste of money [74] or were negative towards robots in general, as they feared that the robot would monitor them or replace them [41, 90]. These findings show how attitude can be influenced by the construct of anxiety, as a fear of the robot can lead to a negative attitude towards robots, and how social influence affects attitude, as the people who were apprehensive towards using the robots could change their mind if encouraged by others.
Regarding attitude as a facilitating factor, six articles reported that the majority of residents were positive about the social robot and its activities [11, 78, 83, 86, 91, 93], and two reported how attitude significantly improved when they used an interactive system design with more sensory modalities [79, 80]. In the case of staff, four articles reported that staff were overall positive or even proud to be involved in the use of social robots [11, 78, 86, 92], and one reported that staff had a positive attitude due to the robots’ positive influence on residents [74], showing a link between perceived usefulness and attitude.
In terms of the relation between attitude and other factors, one article reported that attitudes towards technology could be improved through direct experiences with robots, linking attitude and use, but they found no significant evidence for changes in attitude [82]. Another article reported comments describing a generational difference where older generations may be less likely to accept robots [90], linking attitude to the moderating factor age. Birks et al. reported that the positive attitude of therapists delivering the robot intervention helped them embrace the possibilities of the robot and try to change the attitude of other staff [74].
3.3.6 Perceived Usefulness
This concept was discussed in 18 of the included articles. Perceived usefulness was mostly discussed as a facilitating factor, with a few exceptions. In five articles, social robots were seen as useful for reducing loneliness by increasing social connectedness, as residents had more frequent interactions with other residents, care staff and family members [10, 85]; by giving residents someone to touch and love; by providing comfort and security [81]; by providing friendships [91]; and by interacting with residents like an animal without trying to escape [92]. Communication was a topic closely related to the topic of alleviating loneliness and promoting social connectedness discussed by seven articles. Social robots were reported to lead to increased communication with family members, staff and other residents by providing something to talk about, prompting conversation and eliciting memories to talk about [10, 81, 83, 85, 89, 91, 92]. Social robots also stimulated residents to participate in activities and increased their activity level, which was discussed by five articles: the social robots entertained residents, acted as tools to facilitate activities, provided distractions from boredom and could make the participants more aware and awake [75, 81, 86, 90, 92]. Other usefulness for the residents lies in an increased wellbeing and a positive impact for both people with and without dementia [11, 74, 83]; emotional and therapeutic effects such as comfort, mood improvement and distraction from pain [74, 91, 92]; and the ability to calm and relax residents who were upset, anxious or loud, even complementing/replacing sedatives [74, 81, 92].
Social robots were also reported by nine articles to be useful by providing added value for staff, with staff seeing the robots as applicable in practice and as a tool they could use to better interact with and monitor residents, as well as enabling family members to participate better with value beyond the trial period. In Louie and Nejat’s article, staff found the robots overall useful and had a positive experience overall, linking usefulness and attitude, and Birks et al. reported how therapists working with the robot wanted to show its usefulness to their colleagues [19, 41, 73,74,75, 78, 86, 89, 92]. This is consistent with the findings that the level of engagement impacted perceived usefulness and that the perceived benefits and functionality increased intention to use [41, 82, 94]. This again is in line with the Almere model, which shows that perceived usefulness and perceived ease of use impact intention to use. Three articles linked robot functionalities directly to perceived usefulness—interestingly, Koceski and Koceska found that different applications were found useful by the caregivers (vital signs measurement and reminders) than by residents, who appreciated video conferencing the most [11, 85, 86]. This finding shows that the acceptance of social robots in nursing homes is complicated as different groups of actors—here residents and staff, but in other cases also family members—have different perceptions of what is useful and important and are all important for the acceptance of the robot. Similarly, Robinson et al. reported that family members and staff saw potential in Guide but found that it needed further development and was unsuitable for PlwD at its current stage [92], and Blindheim et al. found that staff found the purpose of the robot unclear, which was a hindering factor resulting in expectations that were not met [75].
3.3.7 Perceived Ease of Use
Seventeen of the included articles reported on perceived ease of use: In terms of facilitating factors, three articles reported that the majority of the residents found the social robot easy to use [10, 85, 89], one found significant improvements in perceived ease of use for the residents who had used the social robot Kabochan [82], and three articles discovered that the staff reported that the robots were easy to use [19, 81, 85, 86]. Mannion et al. described the importance of the design of Mario, including both its appearance and that it is clear to users what the robot is capable of for the ease of use. Chu et al. showed that engagement with the robot Matilda was improved when the robot was made easier to use, e.g., through improving the quality of the voice of the robot, the speed of the robot’s speech and the visibility on the screen of the robot [11, 78].
Factors hindering ease of use included communication issues, with speech patterns, speech-to-text and touchscreens sometimes being challenging for PlwD, especially people with severe dementia [10, 11] and residents having trouble understanding the accent of the robot Matilda [84]. In addition, the age of residents impacted how easy it was for residents to use the robot Mario [11], linking ease of use to the moderating factor age. A challenge for PlwD was that they did not remember using Mario before, but some did improve their ability to interact with Mario over time [11]. Other challenges hindering the ease of use for residents were the size, weight and voice of the robots, Paro’s programming and need to be charged on a regular basis [73, 76, 91, 92], the difficulty of keeping Paro clean [92], the position of the touch screens and the quality of the images on the touch screen on humanoid and telepresence robots [10, 19, 92], and the level of complication of Guide and the large amount of time it took to demonstrate its functions [92]. Additionally, one study mentioned that residents did not find the robot TIAGo very easy to use for older adults, as they are neither good at handling it nor prepared to interact with the robot [94]. Some staff reported that the robots were not easy to use, as staff had to be present, which was difficult to fit with their schedule, the engineers were not always available to assist, the sound volume was too low or staff did not understand robot functionalities, and they underscored the need for staff training and information [11, 75, 90]. Koceski and Koceska found no differences between residents and staff regarding ease of use but found that some functionalities were easier to use than others; telepresence robot navigation was the most difficult functionality, whereas video conference applications were the easiest to use [85], although another article on telepresence robots reported that a resident found it difficult to use the video call function compared to a telephone call [89].
3.3.8 Perceived Enjoyment
Seventeen of the included articles discussed the enjoyment of participants, and they all reported that the participants (both staff and residents) enjoyed using the robots, which was a facilitating factor for the use of the robots [10, 11, 19, 74,75,76,77,78, 81, 83, 84, 86,87,88,89, 91, 93]. Several articles reported that PlwD liked the appearance of the robots, that PlwD enjoyed spending time with them and enjoyed the functionalities of the robots (e.g., music, games), that the robots gave them joy, happiness and a sense of well-being and that the robots could improve the pleasure of PlwD [10, 11, 19, 75, 81, 83, 87, 88, 91, 93]. Staff were also reported to enjoy the use of social robots [19, 75, 81, 86], as well as residents without dementia who were reported to have improved moods, brightening up and dancing spontaneously [74, 76, 77, 84, 86, 89]. One paper described the embodiment of Pepper affording different uses of humour and how the robot was a source of laughter for residents and staff [75].
However, there were also some negative reactions to the robots. Three articles reported that a minority of residents did not enjoy engaging with the robots [10, 83, 87]; e.g., using Mario to look at old photographs led to negative emotions amongst two PlwD when seeing pictures of deceased family members [10], and two residents with dementia at times became agitated or verbally aggressive when introduced to Paro [87]. Three articles reported on a link between robot functionality and the enjoyment of using the robot. Two stated that for PlwD, the pleasure of being with the robot Matilda increased over time due to improvements of the robot’s voice and face recognition and response speed [78, 83]. Louie and Nejat observed one staff member becoming frustrated with the robot, wishing for it to move faster [86], suggesting that improving the functionalities of the robot could facilitate perceived enjoyment.
3.3.9 Trust
Three of the included articles reported briefly on matters of trust. Two articles reported trust as facilitating acceptance; one reported that the robot JustoCat provided its users with feelings of safety and security and reported that the reliability of the social robot both in terms of its technical functions and its presence by the resident’s side was a facilitating factor [81], whereas another reported that privacy was not a concern for the participants using a telepresence robot [89]. One article reported on (lack of) trust as a hindering factor as a staff member felt uncomfortable working with Pepper due to its lack of nonverbal communication in comparison to human colleagues [90].
3.3.10 Social Influence
Eight of the included articles reported results on social influence. In this review, we coded all findings related to family members as social influence, as they are not the primary users of the robot in the nursing home and were not the focus of this review. Therefore, some of the findings here are also of relevance to other categories, such as attitude, but since it relates to family members, we have coded it in this group. Two articles described how the acceptance of both relatives and staff was crucial for the use of robots in nursing homes [11, 82]. This could be both a facilitating and a hindering factor. Six articles reported that family members were mostly positive about social robots, viewing them as improving quality of life in residents and enabling better communication between relatives and residents and seeing the added value of social robot use and in the case of telepresence robots creating a feeling of presence, reassurance and enjoyment for the family [11, 19, 74, 81, 89, 92]; in particular, younger family members interacting with the robot increased the engagement of residents [11]. Mannion et al. further noted that staff and family introducing robots was an advantage [11].
However, some negative reactions were also observed: some family members made derogatory comments about the staff members’ use of Paro [74]; some family members stopped the use of Paro when they observed discomfort in their family member [73]; some family members were concerned about the privacy of the resident when using the telepresence robot Double [89] and relatives thought Guide could use further development, that robots needed to add something extra and that the interactions with Paro were not something for everyone [92]. In line with this, Bemelmans et al. reported that Paro was least successful in supporting family visits compared to other interventions with Paro that did not involve family, mainly due to discomforts reported by the relatives, but they also found that the initial scepticism often turned into enthusiasm during the course of the project [73].
In the context of nursing homes, acceptance is complicated, as it depends on residents, staff and family members. The findings here show that the acceptance of family members is important for the acceptance of robots and is influenced by many different things, such as the attitude or trust of family members.
3.3.11 Facilitating Conditions
Ten of the included articles discussed facilitating conditions. Six articles argued that the training of staff was a crucial facilitating condition for the successful use of social robots in nursing homes. They argued that the intended effects of robot use need to be clear and that staff need to have a foundational understanding of how the robots work, when and for which residents to use them, and how to maintain the robots, including hygiene procedures [19, 73, 74, 79, 86, 87] in one of them, staff were also interested in assistance from volunteers [19]. Gustafsson et al. argued that the ability of JustoCat to fulfil hygiene requirements was a facilitating condition for the staff [81]; here, it is related to the features of the robot, but it is a facilitating condition as the robot fits into the specific hygiene demands in the nursing home environment. Furthermore, two articles emphasized the importance of a quiet environment to use the robot Mario without distractions such as noise, other residents or other activities. This was difficult in a nursing home environment, and they argued that technological advancements are required that enable social robots to communicate and perform speech recognition in noisy environments [10, 11]. Similarly, one article found that a telepresence robot was reliant on a good internet connection but that privacy and security concerns hindered wireless internet access, leaving them reliable on an external modem, which caused connectivity issues [19]. Bemelmans et al. discussed practicalities such as the scheduling of Paro interactions with the other activities of staff, which created difficulties in using Paro [73]. Feng et al. experimented with an interactive system design with more sensory modalities in the nursing home environment and found that an augmented reality display using sounds, touch and visuals on a screen was facilitating conditions that helped capture and maintain the engagement of PlwD [79, 80], something that could also improve the attitude of the residents towards the social robot.
3.3.12 Moderating Factors
Nine of the included articles discussed moderating factors. Health issues were mentioned as both facilitating and hindering social robot use. Birks et al. described how residents with dementia, including those with advanced dementia, responded better to Paro than residents without dementia. This was also the case for residents with depression, disabilities or palliative care needs [74]. Ke et al. found no significant relation between technology acceptance and depression or cognitive function, whereas Mannion et al. reported that people with more severe dementia experienced more difficulties interacting with Mario, and Chen et al. found that physical constraints could hinder the use of Paro [11, 77, 82]. These differences may be related to the types of robots, where a pet robot such as Paro might be easier for people with late-stage dementia to interact with than a humanoid robot such as Mario, which speaks and affords a different kind of interaction.
Three articles reported a lack of technology experience as a hindering factor, but Louie et al. reported that some of the staff thought that their lack of technology experience was a challenge, which the staff themselves expected to improve in the future [11, 82, 86]. In terms of gender, Chu et al. reported that female residents with dementia had more positive engagements with Matilda than male residents, Chen et al. reported that interacting with Paro may go against ideas of masculinity and therefore affect the willingness of men to use it, whereas Ke et al. and Khosla et al. reported that the gender of residents with dementia did not make a significant difference in interactions with Kabochan and Matilda and Tobis et al. only found gender relevant for whether residents found it acceptable that the robot has information about the user, where men were more sceptical towards this after interacting with TIAGo [77, 78, 82, 83, 94]. Two articles mention age as a moderating factor, where older age could be a barrier to interactions with the robots Paro and TIAGo, as residents did not find it suitable for older persons [77, 94].
In addition to these moderating factors, two articles also mentioned the importance of what Birks et al. called normal individual differences and what Moyle et al. 2019 referred to as a person’s biography, such as whether or not a resident liked animals and would therefore show interest in a zoomorphic robot or even the mood of an individual at the certain day and time of the robot interaction. For the latter, Moyle et al. recommended undertaking a brief assessment of the individual resident before using the robot [74, 87].
3.3.13 Intention to Use and Use
We have reported on the actual use of the robots in Table 2 and in the study characteristics. In addition to these findings on how much the robots were used, the papers did not provide results on use as a separate topic. Only two articles reported specifically on intention to use, finding that staff members’ perceptions of the functionality and benefits of Matilda increased their intention to use [41] and that intention to use was scored higher by residents after using the robot TIAGo [94].
3.3.14 Other Themes
As presented in the methods, we also coded using a category called ‘other themes’, to keep an open mind for themes, which were not mentioned in the Almere Model but were of relevance to acceptance. One recurring theme here was how interactions with the social robot(s) encouraged social interactions amongst residents, between residents and staff and between residents and family members. We found results on this in nine papers [10, 11, 74,75,76,77,78,79, 81]. These findings are also closely related to social engagement and are of relevance to the use of technologies and activities in nursing homes, as these are often carried out in group settings in the nursing home [95, 96].
Another theme of relevance to acceptance, that we could not link with the constructs of the Almere model, relates to the design and functionalities of the robots. Sometimes findings on functionalities link with the construct perceived ease of use, perceived usefulness or perceived enjoyment as they related to these categories—in those cases, we have reported the results in those sections of the results. However, some findings on design and functionalities were not linked to the constructs. Four papers reported on this. Khosla et al. described how a combined use of gestures, dance and music improved the acceptance of Matilda [83]. Pu et al. described how the interactive behaviours of Paro made residents engage more positively with the robot [91]. Khaksar et al. described how the newest generation of social robots are able to diagnose, assist and provide company [41], and Barret et al. argued that future robots need to be able to detect emotions and act on them in case PlwD have a negative reaction to interacting with the robot [10].
4 Discussion
In this scoping review, we identified 26 primary articles on the acceptance of social robots in nursing homes. The studies used a wide range of different robots, which provided us with an interesting basis for the review, as these findings apply to a heterogeneous range of social robots in nursing homes. Previous reviews have found that the included studies had very short robot interactions or none at all and have called for more longitudinal studies of social robots in social and health care as well as larger samples [30, 33]. The study length in the included studies varied widely from a single interaction to 5 years. Furthermore, the sample sizes also varied greatly from 3 to 415 research participants, and we observed a growing number of studies with larger samples. Interestingly, more than half of the included articles were published after 2019, showing that this is a growing field of research.
In our review, the included studies were conducted in Europe, Australia, New Zealand, Canada, Japan, Taiwan and Hong Kong. There appears to be a gap in the literature regarding the acceptance of robots in low- or middle-income countries. This may be due to many reasons, such as the costs of social robots, different care systems (e.g., care mainly in the family) and cultural factors (e.g., robot affinity within a society). The WHO estimates that the predicted rise in older adults and PlwD globally will mainly occur in low- and middle-income countries [1, 2], meaning that low- and middle-income countries will have an increased need for new ways of caring for older adults and PlwD. As robots for this group are becoming cheaper with, e.g., low-cost robotic pets showing promising results [97], research on social robots in low- and middle-income countries is a relevant field for future research. Another area for further research is linked to cultural differences and how they impact the acceptance of social robots. Previous studies have found cultural differences in regard to, e.g., attitude toward social robots and argue that these may be grounded in differences in belief systems, but may also be related to how much people have been exposed to robots through media or through interactions with robots. Besides, different perceptions of aging and good care may influence how people perceive social robots for older adults [98, 99]. The articles included in this review did not involve cross-cultural comparisons. This may have impacted our findings on acceptance. Further research on the impact of cultural differences on the acceptance of social robots is needed to understand this phenomenon better.
We will discuss our findings based on the constructs of the Almere model but also address aspects that go beyond the Almere model and contribute to a better understanding of what might be needed to further develop the Almere model of acceptance when studying the acceptance of social robots in a nursing home context. Here, we found that the concept engagement is of interest. Additionally, we identified factors that are relevant for the implementation of social robots in nursing homes, specifically the nursing home context, intervention characteristics and individual users.
4.1 Intention to Use and Trust
We found a large amount of variance in how much the different constructs of the Almere model were discussed in the included articles. Two constructs were rarely studied: intention to use and trust. The few results on intention to use may be related to the fact that the studies addressed the actual use of robots. Trust was originally hypothesized by Heerink et al. to be a direct determinant of intention to use but was the only construct that could not be proven in Heerink et al.’s tests [42]. In this sense, the limited number of results on trust is coherent with the findings from Heerink et al., but it is simultaneously remarkable that trust is so rarely discussed in the literature. In the RAM-care acceptance model, which is based on the Almere Model, Turja et al. found that social influence, attitude, perceived usefulness and perceived enjoyment predicted intention to use, whereas they did not find that trust and ease of use predicted intention to use. Turja et al. nevertheless decided to keep these constructs in the model, as they believed they would become more important as robots become more complex and capable in the future [43]. Working in a nursing home with a vulnerable group of people, many of whom have dementia, dignified and person-centred care are central to interventions in a nursing home [100, 101], and trust from both staff, relatives and residents that the social robots can work ethically with this vulnerable group of people is central. It would therefore be interesting to see more research on trust in social robots used in nursing homes in the future.
4.2 Perceived Usefulness, Perceived Ease of Use and Perceived Enjoyment
In our review, perceived usefulness, perceived ease of use and perceived enjoyment were all studied very frequently and reported findings on both hindering and facilitating factors. Across these three constructs, seeing how robots work well with residents was a facilitating factor for staff, whether the robot improved communication, decreased loneliness, brought joy to residents, calmed agitated residents or generally increased their wellbeing. This is an interesting finding in the context of nursing homes, as the need for the acceptance of the robot from staff, residents and relatives is a factor specific to this context. Furthermore, it shows how the acceptance of one group influences the acceptance of other groups. In the Almere model, this is related to the construct of social influence, where staff and family can affect the acceptance of the older adult, but in our findings, we see that this works interchangeably and that the acceptance of residents can also influence the acceptance of staff and family.
4.3 Engagement
Seeing how robots work well with residents is closely related to engagement, which is not a part of the Almere model of acceptance, but which five of the included papers have used as an outcome measure [79, 82,83,84, 88] and which five papers have included in their study aim [11, 19, 79, 80, 83]. Perugia et al. discuss the importance of engagement when studying people with dementia [95, 96], which is reflected by the fact that all but one of the papers studying engagement focused on PlwD. In our review, we focused on acceptance, but as Perugia et al. pointed out, engaging people with dementia in meaningful activities is important for their well-being on a wide range of parameters. In our results section, we reported how different constructs of the Almere model could improve positive engagement (adaptivity, social presence, perceived sociability, perceived ease of use, social influence and moderating factors) as well as how the level of engagement has an impact on the perceived usefulness. Engagement is therefore also an important measurement in regard to the acceptance of social robots—especially for PlwD.
4.4 Influencing Factor: Intervention Characteristics
In our initial data extraction, some findings of relevance to acceptance were difficult to link with the constructs of the Almere model. Especially findings on the design and functions of the robot, staff training and how social robots encouraged social interactions. It was not immediately clear from the model how to categorize these findings, since design and functions and staff training could also be relevant categories in and of themselves. Koh et al. used the CFIR to understand the implementation of social robots across settings. In their review, most of the identified barriers were related to the domain of “intervention characteristics” [32]. This is interesting, as the design and functions of the robot, which we found challenging to link with the constructs of the Almere model, would fit into this CFIR domain and would be key to understanding barriers to implementation. Papadopoulos et al. did not use an acceptance model in their review on the implementation of humanoid social robots, but interestingly, their findings aligned quite closely with the constructs of the Almere model. When comparing their review findings with the Almere model, the categories familiarization, technical problems and limited capabilities of robots were difficult to match to the Almere model. From the perspective of the CFIR, however, these categories can also be linked to the domain of intervention characteristics. While intervention characteristics are central in both of these reviews and the included papers reported on it, they do not play a clear role in the Almere model. This shows that the current version of the Almere model is not exhaustive and could benefit from an update. Simultaneously, there are relevant elements of the Almere model that Papadopoulos et al. did not describe, such as facilitating conditions, trust, perceived usefulness, anxiety and sociability. They criticized the technology acceptance model for focusing on individual factors only, and since many of their included studies used this model, they reported a lack of evidence on formal and informal carers and factors related to the environment, society, policy and organization [30].
4.5 Influencing Factor: Nursing Home Context
This relates back to our findings from the nursing home context, where we found a need to study the acceptance of residents, staff and family as well as the importance of the organizational context. These factors are partly addressed in the constructs of facilitating conditions and moderating factors in the Almere model, but we argue that they need to be more central when understanding acceptance in nursing homes. In our review, we chose to focus on the acceptance of staff and residents but also found that the acceptance of family members is important and that different constructs influence this acceptance as well. In the review, we discuss this as social influence, but looking at, e.g., the attitudes, anxieties, trust, and perceived usefulness of family members is also relevant in itself, specifically in the nursing home context. Furthermore, we found that there were sometimes differences in the needs and priorities of residents and staff, for example, in terms of anxiety and usefulness—something that is important to take into account when designing and implementing social robots for a nursing home population. In line with our review findings, Whelan et al. found that the different user groups are important in the nursing home, and that their opinions may differ. It might be of interest to conduct research into whether acceptance models look the same for staff, residents and family or if different constructs are relevant for the different actors in the nursing home.
We also found that robots need to be compatible with dignified care and that staff training is of importance—which can be a problem as nursing homes are characterized by a high workload for the staff, and as shown in the beginning, this will only increase as there will be more older adults in need of care and not enough staff to care for them. Another aspect of importance in nursing homes is the practicalities of everyday life in an institutional home. Many of the hindering factors found across the Almere constructs are centred on practical everyday issues such as storage, internet connection and hygiene. These findings show the importance of adapting the intervention with social robots to the organizational context of the nursing home.
4.6 Influencing Factor: The Individual
Residents of nursing homes are a diverse user group with different health problems, disabilities and cognitive levels; as these factors continue to change for individual residents and as nursing homes have relatively high resident turnover, adaptivity is a highly relevant topic. Papadopoulos et al. described robots’ lack of adaptability as a central barrier to implementation and reported personalization of a robot as one of the primary enablers of implementation [30], which relates back to our findings on the importance of the design and the functions of social robots. Similarly, Whelan et al. argued that robots used in residential care have to adapt to the needs of a range of users with different needs as well as cognitive and physical limitations to ensure the perceived ease of use [33]. Here our findings differed slightly, as we found links between the perceived adaptivity, perceived enjoyment and perceived usefulness, but not the perceived ease of use.
It is also important to keep in mind the potential vulnerability of this group and some of the ethical risks when introducing social robots to people with dementia. Sætra discussed the ethics of using social robots for people with dementia using the concept of the Turing test to discuss the different degrees to which people interacting with the robots believe that they are real or alive. Sætra argues that we have to be careful, as the social robots may deceive PlwD into believing that Paro for example, is a real animal or even if they do not believe it to be real they may still subconsciously react to it as if it was real—what he calls passing the subconscious Turing test [102]. On the other hand, Koh et al. found that the realisticness of the robots and the residents perceiving them as animals and building emotional connections with them, was experienced as positive by care professionals [103]. Our results on anxiety show that there is a risk that PlwD can end up caring too much for the robots, which can lead to anxiety and worries about the robot. Paradoxically, it seems that too much acceptance of the pet robot as a social being and a companion can here be negative for the PlwD. This is important to think of when looking at social presence and sociability when designing and implementing for this specific group.
4.7 Recommendations for Further Research
Based on our review findings, we recommend further research into three areas of acceptance of social robots. First of all, we recommend that the Almere model of acceptance is expanded deepening our knowledge on the intervention characteristics; the different user groups of residents, staff and relatives; the nursing home context; and the concept of engagement—aspects, which were important for the acceptance of social robots in the included papers. Second of all, we recommend studies that compare findings on acceptance across cultures, to gain more knowledge on how cultural factors impact the acceptance of social robots. Thirdly, we recommend research to look not only at high income countries, but also low- and middle income countries. Something which may be more feasible, now that some robots (such as low cost robotic pets) are becoming cheaper and more available.
5 Strengths and Limitations
We chose the scoping review methodology because the use of social robots in nursing homes is a fairly new and expanding research field, and we wanted to capture all the relevant literature across different research designs. We have followed the scoping review methodology guidelines outlined by Arksey and O’Malley, Levac et al. and the JBI manual for evidence synthesis on scoping reviews [46,47,48]. To our knowledge, this was the first review with a systematic approach focusing on the acceptance of social robots based on the Almere model in the context of nursing homes and looking into factors facilitating and hindering acceptance. To do so, a scoping review is deemed highly appropriate.
A formal assessment of study quality was not required based on the applied scoping review methodology and was not conducted. Nevertheless, an assessment of study quality could have strengthened the findings and helped interpret them based on the quality of the studies. Quantitative assessment of the coding process was not performed due to the iterative coding process, where we had several rounds discussing the coding with the co-authors, which lead to codes being reassigned to ensure a reliable coding. Furthermore, as conference proceedings were excluded in this review due to resource constraints and our inclusion criteria, some studies may have been omitted from this review.
The Almere model of acceptance proved useful in understanding the phenomenon of acceptance of social robots in nursing homes. It enabled us to capture many different aspects of acceptance in the included papers. There are also limits to using this model for our review however and the model may have limited our findings, as other terms of relevance to acceptance were identified but were not part of our search string.
6 Conclusion
The aim of this scoping review was to provide a picture of factors facilitating and hindering the acceptance of social robots based on the Almere model in nursing homes identified in the literature, to identify which factors and aspects of acceptance have not been researched and to consequentially identify research gaps. We found results on all constructs of the Almere model of acceptance as well as hindering and/or facilitating factors for each construct. Perceived usefulness, perceived ease of use and perceived enjoyment were the most studied constructs. Across several constructs, seeing robots positively impacting residents was one of the key facilitating factors, and practical difficulties were usually a hindering factor. Both crosscutting themes are related to the complexity of the nursing home context, where staff, residents and relatives are important actors and where practicalities are important in busy everyday institutional life. It is important for HRI research and implementation research to understand these different organizational aspects as well as the specificities and diversities of user groups when social robots are being designed for as well as used and implemented in nursing homes. We found that trust was amongst the least studied constructs but believe this to be of great importance in the context of nursing homes and dementia and call for more studies on this in the future.
Although the Almere model proved useful for our review, we have raised some critiques of the model. There is a need to look at different user groups in the context of nursing homes and maybe even have specific acceptance models for each user group. Some Almere model constructs had findings on both facilitating and hindering factors, while others only had findings that were either facilitating or hindering. We argue that this is partly related to the framing of the constructs in the Almere model and their inherent valuations. It is not surprising that anxiety had findings on hindering factors, as anxiety is inherently a negative construct. Trust, on the other hand, as a positive concept, mainly provides facilitating factors. The constructs are not on the same level and are not all framed as neutral constructs but rather already have an inherent evaluation in them, which can lead to a bias in the findings and is something we found challenging when working with the Almere model for our review.
We have furthermore discussed other concepts and factors of relevance to the acceptance of social robots in nursing homes, such as engagement, the nursing home context, the design and functionalities of the robot and the individual users. For future research, it would be relevant to look into defining a new acceptance model for social robots that takes these findings into account. More studies are needed to fill the gaps identified in the literature and to expand our understanding of the acceptance of social robots in nursing homes and ensure high-quality evidence to support social robot interventions in nursing homes.
Data Availability
In Online Resources 1 and 2, we provide the search string as well as the list of inclusion and exclusion criteria that were used for the screening of the articles. The funding sources of the included articles can be found in Online Resource 3. In Online Resource 4, we provide a completed PRISMA-ScR guideline. In Online Resource 5, we provide the code book used for data extraction, and in Online Resource 6, we provide examples of how we coded the articles. The protocol was registered with the Open Science Framework (https://osf.io/6zxfp).
Code Availability
Not applicable.
Notes
We use the term construct for all the concepts in the Almere model, as this is the term the authors use themselves. Others have used the terms concepts or determinants, but we will use the terminology of Heerink et al. in this review.
References
World Health Organization (2021) Ageing. 2021 [23.07.2021]. https://www.who.int/health-topics/ageing#tab=tab_1
World Health Organization (2021) Dementia. 2021 02.09.2021[07.06.2022]. https://www.who.int/news-room/fact-sheets/detail/dementia
Spasova S et al (2018) Challenges in long-term care in Europe: a study of national policies. Eur Comm. https://doi.org/10.2767/84573
Heerink M (2010) Assessing acceptance of assistive social robots by aging adults. In: Faculty of Science: Informatics Institute Universiteit van Amsterdam [Host], Amsterdam
Naneva S, Sarda Gou M, Webb TL, Prescott TJ (2020) A systematic review of attitudes, anxiety, acceptance, and trust towards social robots. Int J Soc Robot 12(6):1179–1201. https://doi.org/10.1007/s12369-020-00659-4
Duffy BR (2003) Anthropomorphism and the social robot. Robot Auton Syst 42(3):177–190. https://doi.org/10.1016/S0921-8890(02)00374-3
Jøranson N, Pedersen I, Rokstad AMM, Ihlebæk C (2016) Change in quality of life in older people with dementia participating in Paro-activity: a cluster-randomized controlled trial. J Adv Nurs 72(12):3020–3033. https://doi.org/10.1111/jan.13076
Libin A, Cohen-Mansfield J (2004) Therapeutic robocat for nursing home residents with dementia: preliminary inquiry. Am J Alzheimers Dis Other Demen 19(2):111–116. https://doi.org/10.1177/153331750401900209
Tamura T et al (2004) Is an entertainment robot useful in the care of elderly people with severe dementia? J Gerontol A Biol Sci Med Sci 59(1):M83–M85. https://doi.org/10.1093/gerona/59.1.m83
Barrett E et al (2019) Evaluation of a companion robot for individuals with dementia: quantitative findings of the MARIO project in an irish residential care setting. J Gerontol Nurs 47(7):36–45. https://doi.org/10.3928/00989134-20190531-01
Mannion A et al (2019) Introducing the social robot MARIO to people living with dementia in long term residential care: reflections. Int J Soc Robot. https://doi.org/10.1007/s12369-019-00568-1
Casey D, Murphy K, Oscar J (2016) Designing an acceptable and useful companion robot for people with dementia and carers in Ireland: the MARIO project. https://doi.org/10.13025/S85W4H
Blond L (2018) Dances with robots: understanding social robots in practice. Aarhus Universitet, SUN-TRYK
Blond L (2019) Studying robots outside the lab: HRI as ethnography. Paladyn J Behav Robot 10(1):117–127. https://doi.org/10.1515/pjbr-2019-0007
Leeson C (2017) Anthropomorphic robots on the move: a transformative trajectory from Japan to Danish Healthcare. PhD Dissertation University of Copenhagen
Strandbech JD (2018) Humanoid robots for health and welfare. Aalb Univ. https://doi.org/10.5278/vbn.phd.hum.00092
Bechade L, Dubuisson-Duplessis G, Pittaro G, Garcia M, Devillers L (2019) Towards metrics of evaluation of pepper robot as a social companion for the elderly. In: Eskenazi M, Devillers L, Mariani J (eds) Advanced social interaction with agents. 8th International workshop on spoken dialog systems. Springer, Cham. pp 89–101. https://doi.org/10.1007/978-3-319-92108-2_11
Sato M et al (2020) Rehabilitation care with Pepper humanoid robot: a qualitative case study of older patients with schizophrenia and/or dementia in Japan. Enferm Clin 30(Suppl 1):32–36. https://doi.org/10.1016/j.enfcli.2019.09.021
Moyle W et al (2014) Connecting the person with dementia and family: a feasibility study of a telepresence robot. BMC Geriatr 14(1):7. https://doi.org/10.1186/1471-2318-14-7
Fattal C et al (2020) Perspectives on usability and accessibility of an autonomous humanoid robot living with elderly people. Disabil Rehabil Assist Technol. https://doi.org/10.1080/17483107.2020.1786732
Frennert S, Östlund B (2014) Review: seven matters of concern of social robots and older people. Int J Soc Robot 6(2):299–310. https://doi.org/10.1007/s12369-013-0225-8
Giaretta A, De Donno M, Dragoni N (2018) Adding salt to pepper: a structured security assessment over a humanoid robot. In: Proceedings of the 13th international conference on availability, reliability and security. ACM. https://doi.org/10.1145/3230833.3232807
Mordoch E, Osterreicher A, Guse L, Roger K, Thompson G (2013) Use of social commitment robots in the care of elderly people with dementia: a literature review. Maturitas 74(1):14–20. https://doi.org/10.1016/j.maturitas.2012.10.015
Pedersen I, Reid S, Aspevig K (2018) Developing social robots for aging populations: a literature review of recent academic sources. Sociol Compass 12(6):e12585. https://doi.org/10.1111/soc4.12585
Gongora Alonso S et al (2019) Social robots for people with aging and dementia: a systematic review of literature. Telemed J E-Health 25(7):533–540. https://doi.org/10.1089/tmj.2018.0051
Bemelmans R, Gelderblom GJ, Jonker P, de Witte L (2012) Socially assistive robots in elderly care: a systematic review into effects and effectiveness. J Am Med Dir Assoc 13(2):114-120.e1. https://doi.org/10.1016/j.jamda.2010.10.002
Maalouf N, Sidaoui A, Elhajj IH, Asmar D (2018) Robotics in nursing: a scoping review. J Nurs Scholarsh 50(6):590–600. https://doi.org/10.1111/jnu.12424
Kangasniemi M, Karki S, Colley N, Voutilainen A (2019) The use of robots and other automated devices in nurses’ work: an integrative review. Int J Nurs Pract 25(4):e12739. https://doi.org/10.1111/ijn.12739
Abdi J, Al-Hindawi A, Ng T, Vizcaychipi MP (2018) Scoping review on the use of socially assistive robot technology in elderly care. BMJ Open 8(2):e018815. https://doi.org/10.1136/bmjopen-2017-018815
Papadopoulos I, Koulouglioti C, Lazzarino R, Ali S (2020) Enablers and barriers to the implementation of socially assistive humanoid robots in health and social care: a systematic review. BMJ Open 10(1):e033096. https://doi.org/10.1136/bmjopen-2019-033096
Ozdemir D, Cibulka J, Stepankova O, Holmerova I (2021) Design and implementation framework of social assistive robotics for people with dementia—a scoping review. Health Technol 11(2):367–378. https://doi.org/10.1007/s12553-021-00522-0
Koh WQ, Felding SA, Budak KB, Toomey E, Casey D (2021) Barriers and facilitators to the implementation of social robots for older adults and people with dementia: a scoping review. BMC Geriatr 21(1):351. https://doi.org/10.1186/s12877-021-02277-9
Whelan S et al (2018) Factors affecting the acceptability of social robots by older adults including people with dementia or cognitive impairment: a literature review. Int J Soc Robot 10(5):643–668. https://doi.org/10.1007/s12369-018-0471-x
Sanford AM et al (2015) An international definition for “nursing home.” J Am Med Dir Assoc 16(3):181–184. https://doi.org/10.1016/j.jamda.2014.12.013
Alexandre B, Reynaud E, Osiurak F, Navarro J (2018) Acceptance and acceptability criteria: a literature review. Cogn, Technol Work 20(2):165–177. https://doi.org/10.1007/s10111-018-0459-1
Davis FD (1986) A technology acceptance model for empirically testing new end-user information systems: theory and results. Massachusetts Institute of Technology
Davis FD, Bagozzi RP, Warshaw PR (1989) User acceptance of computer technology: a comparison of two theoretical models. Manag Sci 35(8):982–1003
Ghazali AS, Ham J, Barakova E, Markopoulos P (2020) Persuasive robots acceptance model (PRAM): roles of social responses within the acceptance model of persuasive robots. Int J Soc Robot. https://doi.org/10.1007/s12369-019-00611-1
Tamilmani K, Rana NP, Wamba SF, Dwivedi R (2021) The extended Unified Theory of Acceptance and Use of Technology (UTAUT2): a systematic literature review and theory evaluation. Int J Inf Manag 57:102269. https://doi.org/10.1016/j.ijinfomgt.2020.102269
Chen K, Chan AHS (2014) Gerontechnology acceptance by elderly Hong Kong Chinese: a senior technology acceptance model (STAM). Ergonomics 57(5):635–652. https://doi.org/10.1080/00140139.2014.895855
Khaksar SMS, Khosla R, Singaraju S, Slade B (2019) Carer’s perception on social assistive technology acceptance and adoption: moderating effects of perceived risks. Behav Inf Technol. https://doi.org/10.1080/0144929X.2019.1690046
Heerink M, Kröse B, Evers V, Wielinga B (2010) Assessing acceptance of assistive social agent technology by older adults: the Almere model. Int J Soc Robot 2(4):361–375. https://doi.org/10.1007/s12369-010-0068-5
Turja T, Aaltonen I, Taipale S, Oksanen A (2020) Robot acceptance model for care (RAM-care): a principled approach to the intention to use care robots. Inf Manag 57(5):103220. https://doi.org/10.1016/j.im.2019.103220
Tricco A, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MD, Horsley T, Weeks L, Hempel S (2018) PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 169(7):467–473. https://doi.org/10.7326/m18-0850
Arksey H, O’Malley L (2005) Scoping studies: towards a methodological framework. Int J Soc Res Methodol 8(1):19–32. https://doi.org/10.1080/1364557032000119616
Levac D, Colquhoun H, O’Brien KK (2010) Scoping studies: advancing the methodology. Implement Sci 5(1):69. https://doi.org/10.1186/1748-5908-5-69
Peters MD et al (2015) Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 13(3):141–146. https://doi.org/10.1097/XEB.0000000000000050
Peters M, et al (2020) Chapter 11: scoping reviews. In: Aromataris E, Munn Z (eds) JBI manual for evidence synthesis. JBI. https://doi.org/10.46658/JBIMES-20-12
UNHCR (2023) Older persons. 2023 [19.01.2023]; 2.4. https://emergency.unhcr.org/entry/43935/older-persons
Alzheimer Europe (2021) Dementia. 2021. https://www.alzheimer-europe.org/dementia
Taylor JS, DeMers SM, Vig EK, Borson S (2012) The disappearing subject: exclusion of people with cognitive impairment and dementia from geriatrics research. J Am Geriatr Soc 60(3):413–419. https://doi.org/10.1111/j.1532-5415.2011.03847.x
Brooks J, Savitch N, Gridley K (2017) Removing the ‘gag’—involving people with dementia in research as advisers and participants. Soc Res Prac 3:3–14
McGowan J et al (2016) PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol 75:40–46. https://doi.org/10.1016/j.jclinepi.2016.01.021
The EndNote Team (2013) EndNote. Clarivate, Philadelphia
Covidence Covidence systematic review software. Veritas Health Innovation, Melbourne, Australia
Elo S, Kyngäs H (2008) The qualitative content analysis process. J Adv Nurs 62(1):107–115. https://doi.org/10.1111/j.1365-2648.2007.04569.x
VERBI Software (2022) MAXQDA. Verbi Software, Berlin
Venkatesh V, Morris MG, Davis GB, Davis FD (2003) User acceptance of information technology: toward a unified view. MIS Q 27(3):425–478. https://doi.org/10.2307/30036540
Kachouie R, Sedighadeli S, Khosla R, Chu M-T (2014) Socially assistive robots in elderly care: a mixed-method systematic literature review. Int J Hum Comput Interact 30(5):369–393. https://doi.org/10.1080/10447318.2013.873278
Abbott R et al (2019) How do “robopets” impact the health and well-being of residents in care homes? A systematic review of qualitative and quantitative evidence. Int J Older People Nurs 14(3):e12239. https://doi.org/10.1111/opn.12239
Bedaf S, Marti P, Amirabdollahian F, de Witte L (2018) A multi-perspective evaluation of a service robot for seniors: the voice of different stakeholders. Disabil Rehabil Assist Technol 13(6):592–599. https://doi.org/10.1080/17483107.2017.1358300
Broekens J, Heerink M, Rosendal H (2009) Assistive social robots in elderly care: a review. Gerontechnology 8(2):94–103. https://doi.org/10.4017/gt.2009.08.02.002.00
Chen S-C, Jones C, Moyle W (2018) Social robots for depression in older adults: a systematic review. J Nurs Scholarsh 50(6):612–622. https://doi.org/10.1111/jnu.12423
Scoglio AA, Reilly ED, Gorman JA, Drebing CE (2019) Use of social robots in mental health and well-being research: systematic review. J Med Internet Res 21(7):e13322. https://doi.org/10.2196/13322
Vandemeulebroucke T, de Casterlé BD, Gastmans C (2018) How do older adults experience and perceive socially assistive robots in aged care: a systematic review of qualitative evidence. Aging Ment Health 22(2):149–167. https://doi.org/10.1080/13607863.2017.1286455
Jones C, Liu F, Murfield J, Moyle W (2020) Effects of non-facilitated meaningful activities for people with dementia in long-term care facilities: a systematic review. Geriatr Nurs 41(6):863–871. https://doi.org/10.1016/j.gerinurse.2020.06.001
Choi HK, Lee SH (2021) Trends and effectiveness of ICT interventions for the elderly to reduce loneliness: a systematic review. Healthcare 9(3):293. https://doi.org/10.3390/healthcare9030293
Scerri A, Sammut R, Scerri C (2021) Formal caregivers’ perceptions and experiences of using pet robots for persons living with dementia in long-term care: a meta-ethnography. J Adv Nurs 77(1):83–97. https://doi.org/10.1111/jan.14581
Vandemeulebroucke T, Dzi K, Gastmans C (2021) Older adults’ experiences with and perceptions of the use of socially assistive robots in aged care: a systematic review of quantitative evidence. Arch Gerontol Geriatr 95:104399. https://doi.org/10.1016/j.archger.2021.104399
Wang X, Shen J, Chen Q (2021) How PARO can help older people in elderly care facilities: a systematic review of RCT. Int J Nurs Knowl. https://doi.org/10.1111/2047-3095.12327
Loveys K et al (2022) Artificial intelligence for older people receiving long-term care: a systematic review of acceptability and effectiveness studies. Lancet Healthy Longev 3(4):e286–e297. https://doi.org/10.1016/s2666-7568(22)00034-4
Lu L-C et al (2021) Effectiveness of companion robot care for dementia: a systematic review and meta-analysis. Innov Aging. https://doi.org/10.1093/geroni/igab013
Bemelmans R, Gelderblom GJ, Jonker P, de Witte L (2016) How to use robot interventions in intramural psychogeriatric care; a feasibility study. Appl Nurs Res 30:154–157. https://doi.org/10.1016/j.apnr.2015.07.003
Birks M, Bodak M, Barlas J, Harwood J, Pether M (2016) Robotic seals as therapeutic tools in an aged care facility: a qualitative study. J Aging Res 2016:8569602. https://doi.org/10.1155/2016/8569602
Blindheim K, Solberg M, Hameed IA, Alnes RE (2022) Promoting activity in long-term care facilities with the social robot Pepper: a pilot study. Inform Health Soc Care. https://doi.org/10.1080/17538157.2022.2086465
Bradwell HL et al (2021) User-centered design of companion robot pets involving care home resident-robot interactions and focus groups with residents, staff, and family: qualitative study. JMIR Rehabil Assist Technol 8(4):e30337. https://doi.org/10.2196/30337
Chen S-C et al (2022) Can the Paro be my Buddy? Meaningful experiences from the perspectives of older adults. Geriatr Nurs 43:130–137. https://doi.org/10.1016/j.gerinurse.2021.11.011
Chu M-T, Khosla R, Khaksar SMS, Nguyen K (2017) Service innovation through social robot engagement to improve dementia care quality. Assist Technol 29(1):8–18. https://doi.org/10.1080/10400435.2016.1171807
Feng Y et al (2022) Context-enhanced human–robot interaction: exploring the role of system interactivity and multimodal stimuli on the engagement of people with dementia. Int J Soc Robot 14(3):807–826. https://doi.org/10.1007/s12369-021-00823-4
Feng Y, Barakova EI, Yu S, Hu J, Rauterberg GWM (2020) Effects of the level of interactivity of a social robot and the response of the augmented reality display in contextual interactions of people with dementia. Sensors 20(13):3771. https://doi.org/10.3390/s20133771
Gustafsson C, Svanberg C, Müllersdorf M (2015) Using a robotic cat in dementia care: a pilot study. J Gerontol Nurs 41(10):46–56. https://doi.org/10.3928/00989134-20150806-44
Ke C, Lou VW-Q, Tan KC-K, Wai MY, Chan LL (2020) Changes in technology acceptance among older people with dementia: the role of social robot engagement. Int J Med Inform 141:104241. https://doi.org/10.1016/j.ijmedinf.2020.104241
Khosla R, Nguyen K, Chu M-T (2017) Human robot engagement and acceptability in residential aged care. Int J Hum Comput Interact 33(6):510–522. https://doi.org/10.1080/10447318.2016.1275435
Khosla R, Chu M-T (2013) Embodying care in matilda: an affective communication robot for emotional wellbeing of older people in australian residential care facilities. ACM Trans Manag Inf Syst 4(4):18. https://doi.org/10.1145/2544104
Koceski S, Koceska N (2016) Evaluation of an assistive telepresence robot for elderly healthcare. J Med Syst 40(5):121. https://doi.org/10.1007/s10916-016-0481-x
Louie W-YG, Nejat G (2020) A social robot learning to facilitate an assistive group-based activity from non-expert caregivers. Int J Soc Robot 12(5):1159–1176. https://doi.org/10.1007/s12369-020-00621-4
Moyle W et al (2019) Using a therapeutic companion robot for dementia symptoms in long-term care: reflections from a cluster-RCT. Aging Ment Health 23(3):329–336. https://doi.org/10.1080/13607863.2017.1421617
Moyle W et al (2017) Use of a robotic seal as a therapeutic tool to improve dementia symptoms: a cluster-randomized controlled trial. J Am Med Dir Assoc 18(9):766–773. https://doi.org/10.1016/j.jamda.2017.03.018
Niemelä M, van Aerschot L, Tammela A, Aaltonen I, Lammi H (2021) Towards ethical guidelines of using telepresence robots in residential care. Int J Soc Robot 13(3):431–439. https://doi.org/10.1007/s12369-019-00529-8
Papadopoulos I et al (2022) A qualitative exploration of care homes workers’ views and training needs in relation to the use of socially assistive humanoid robots in their workplace. Int J Older People Nurs 17(3):e12432. https://doi.org/10.1111/opn.12432
Pu L, Moyle W, Jones C (2020) How people with dementia perceive a therapeutic robot called PARO in relation to their pain and mood: a qualitative study. J Clin Nurs 29(3–4):437–446. https://doi.org/10.1111/jocn.15104
Robinson H, MacDonald BA, Kerse N, Broadbent E (2013) Suitability of healthcare robots for a dementia unit and suggested improvements. J Am Med Dir Assoc 14(1):34–40. https://doi.org/10.1016/j.jamda.2012.09.006
Sumioka H, Yamato N, Shiomi M, Ishiguro H (2021) A minimal design of a human infant presence: a case study toward interactive doll therapy for older adults with dementia. Front Robot AI. https://doi.org/10.3389/frobt.2021.633378
Tobis S, Piasek J, Cylkowska-Nowak M, Suwalska A (2022) Robots in eldercare: how does a real-world interaction with the machine influence the perceptions of older people? Sensors 22(5):1717. https://doi.org/10.3390/s22051717
Perugia G et al (2018) Understanding engagement in dementia through behavior. The Ethographic and Laban-Inspired Coding System of Engagement (ELICSE) and the Evidence-Based Model of Engagement-Related Behavior (EMODEB). Front Psychol. https://doi.org/10.3389/fpsyg.2018.00690
Perugia G et al (2022) ENGAGE-DEM: a model of engagement of people with dementia. IEEE Trans Affect Comput 13(2):926–943. https://doi.org/10.1109/TAFFC.2020.2980275
Koh WQ, Ang FXH, Casey D (2021) Impacts of low-cost robotic pets for older adults and people with dementia: scoping review. JMIR Rehabil Assist Technol 8(1):e25340. https://doi.org/10.2196/25340
Broadbent E, Stafford R, MacDonald B (2009) Acceptance of healthcare robots for the older population: review and future directions. Int J Soc Robot 1(4):319. https://doi.org/10.1007/s12369-009-0030-6
de Graaf MMA, Ben Allouch S (2013) Exploring influencing variables for the acceptance of social robots. Robot Auton Syst 61(12):1476–1486. https://doi.org/10.1016/j.robot.2013.07.007
Vernooij-Dassen M, Moniz-Cook E (2016) Person-centred dementia care: moving beyond caregiving. Aging Ment Health 20(7):667–668. https://doi.org/10.1080/13607863.2016.1154017
Backman A et al (2020) Embodying person-centred being and doing: Leading towards person-centred care in nursing homes as narrated by managers. J Clin Nurs 29(1–2):172–183. https://doi.org/10.1111/jocn.15075
Sætra HS (2022) First, they came for the old and demented. Hum Arenas 5(1):25–43. https://doi.org/10.1007/s42087-020-00125-7
Koh WQ, Vandemeulebroucke T, Gastmans C, Miranda R, Van den Block L (2023) The ethics of pet robots in dementia care settings: care professionals’ and organisational leaders’ ethical intuitions. Front Psychiatry. https://doi.org/10.3389/fpsyt.2023.1052889
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by the European Union’s Horizon 2020, Marie Skłodowska-Curie Actions—Innovative Training Network under Grant Agreement No. 813196.
Author information
Authors and Affiliations
Contributions
SAF conceptualized the review approach, developed the review design with continuous input from WQK, ST, KBB, FLU and MR and conducted the literature search as well as the hand search. SAF and WQK performed the screening, study selection and data extraction with input from ST and MR when a third opinion was needed. The data synthesis and review writing were led by SAF with meaningful contributions from WQK, ST, KBB, FLU and MR. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
There are no conflicts of interest.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Felding, S.A., Koh, W.Q., Teupen, S. et al. A Scoping Review Using the Almere Model to Understand Factors Facilitating and Hindering the Acceptance of Social Robots in Nursing Homes. Int J of Soc Robotics 15, 1115–1153 (2023). https://doi.org/10.1007/s12369-023-01012-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12369-023-01012-1