
Abstract
Background
Primary cardiac lymphoma (PCL) and primary cardiac sarcoma (PCS) are similar in clinical presentation but differ in management and outcomes. We aim to explore the role of PET morphology and clinical characteristics in distinguishing PCL from PCS.
Methods
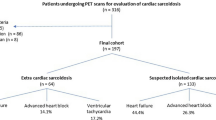
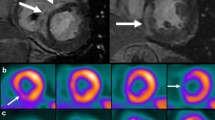
Pretreatment 18F-FDG PET/CT and contrast-enhanced CT were performed in PCL (n = 14) and PCS (n = 15) patients. Patient demographics, overall survival, and progression-free survival were reviewed. PET/CT morphological and metabolic features were extracted. Specifically, R_Kurtosis, a PET-morphology parameter reflecting the tumor expansion within the heart, was calculated.
Results
Compared with PCS, PCL occurred at an older age, resulted in more cardiac dysfunctions and arrhythmias, and showed higher glucometabolism (SUVmax, SUVpeak, SUVmean, MTV, and TLG). Curative treatments improved survival for PCL but not for PCS. Multivariable logistic regression identified R_Kurtosis (OR = 27.025, P = .007) and cardiac conduction disorders (OR = 37.732, P = .016) independently predictive of PCL, and classification and regression tree analysis stratified patients into three subgroups: R_Kurtosis ≥ 0.044 (probability of PCL 88.9%), R_Kurtosis < 0.044 with conduction disorders (80.0%), and R_Kurtosis < 0.044 without conduction disorders (13.3%).
Conclusion
PET-derived tumor expansion pattern (R_Kurtosis) and cardiac conduction disorders were helpful in distinguishing PCL from PCS, which might assist the clinical management.





Similar content being viewed by others

Abbreviations
- PCS:
-
Primary cardiac sarcoma
- PCL:
-
Primary cardiac lymphoma
- CECT:
-
Contrast-enhanced CT
- MTV:
-
Metabolic tumor volume
- TLG:
-
Total lesion glycolysis
- OS:
-
Overall survival
- PFS:
-
Progression-free survival
- HR:
-
Hazard ratio
- CART:
-
Classification and regression tree
- LVEF:
-
Left ventricular ejection fraction
References
Sultan I, Bianco V, Habertheuer A, Kilic A, Gleason TG, Aranda-Michel E. Long-term outcomes of primary cardiac malignancies: Multi-institutional results from the National Cancer Database. J Am Coll Cardiol 2020;75:2338‐47.
Yin K, Brydges H, Lawrence KW, Wei Y, Karlson KJ, McAneny DB, et al. Primary cardiac lymphoma. J Thorac Cardiovasc Surg 2020. https://doi.org/10.1016/j.jtcvs.2020.09.102.
Wei XJ, Yuan H, Khong PL, Zhang F, Liao PJ, Jiang XM, et al. Primary cardiac lymphoma: The management and outcome of a single-centre cohort of 22 patients. Acta Oncol 2021;60:1122‐9.
Chen H, Qian S, Shi P, Liu L, Yang F. A presentation, treatment, and survival analysis of primary cardiac lymphoma cases reported from 2009 to 2019. Int J Hematol 2020;112:65‐73.
Maleszewski JJ, Anavekar NS, Moynihan TJ, Klarich KW. Pathology, imaging, and treatment of cardiac tumours. Nat Rev Cardiol 2017;14:536‐49.
Francis R, Lewis C. Myocardial biopsy: techniques and indications. Heart 2018;104:950‐8.
Liu ET, Sun TT, Dong HJ, Wang SY, Chen ZR, Liu C, et al. Combined PET/CT with thoracic contrast-enhanced CT in assessment of primary cardiac tumors in adult patients. EJNMMI Res 2020;10:75.
Liu E, Huang J, Dong H, Chen Z, Liu C, Xie Q, et al. Diagnostic challenges in primary cardiac lymphoma, the opportunity of (18)F-FDG PET/CT integrated with contrast-enhanced CT. J Nucl Cardiol 2021. https://doi.org/10.1007/s12350-021-02723-6.
Chareonthaitawee P, Beanlands RS, Chen W, Dorbala S, Miller EJ, Murthy VL, et al. Joint SNMMI–ASNC expert consensus document on the role of 18F-FDG PET/CT in cardiac sarcoid detection and therapy monitoring. J Nucl Cardiol 2017;24:1741‐58.
Kaalep A, Sera T, Rijnsdorp S, Yaqub M, Talsma A, Lodge MA, et al. Feasibility of state of the art PET/CT systems performance harmonisation. Eur J Nucl Med Mol Imaging 2018;45:1344‐61.
van Griethuysen JJM, Fedorov A, Parmar C, Hosny A, Aucoin N, Narayan V, et al. Computational radiomics system to decode the radiographic phenotype. Cancer Res 2017;77:e104‐7.
Klabunde RE. Cardiac electrophysiology: Normal and ischemic ionic currents and the ECG. Adv Physiol Educ 2017;41:29‐37.
Harris FE. Chapter 6—Multidimensional problems. In: Harris FE, editor. Mathematics for physical science and engineering. Boston: Elsevier; 2014. p. 195‐227.
Mishra P, Pandey CM, Singh U, Gupta A, Sahu C, Keshri A. Descriptive statistics and normality tests for statistical data. Ann Card Anaesth 2019;22:67‐72.
Joanes DN, Gill CA. Comparing measures of sample skewness and kurtosis. J R Stat Soc D 1998;47:183‐9.
Kavakbasi E, Scheld HH, Kessler T, Sindermann JR, Kosek V, Tjan TDT, et al. Postoperative complications and long-term results after primary cardiac sarcoma resection. Thorac Cardiovasc Surg 2018;66:637‐44.
Hubeaux S, Rufibach K. SurvRegCensCov: Weibull regression for a right-censored endpoint with a censored covariate. arXiv preprint 2014. arXiv:14020432.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J R Stat Soc B 1995;57:289‐300.
Asadian S, Rezaeian N, Hosseini L, Toloueitabar Y, Hemmati Komasi MM. The role of cardiac CT and MRI in the diagnosis and management of primary cardiac lymphoma: A comprehensive review. Trends Cardiovasc Med 2021. https://doi.org/10.1016/j.tcm.2021.08.010.
Motwani M, Kidambi A, Herzog BA, Uddin A, Greenwood JP, Plein S. MR imaging of cardiac tumors and masses: A review of methods and clinical applications. Radiology 2013;268:26‐43.
Niclauss L, Montemurro M, Kirsch M, Pretre R. Sarcoma of the heart: Survival after surgery. Interact Cardiovasc Thorac Surg 2018;27:198‐201.
Smrke A, Wang Y, Simmons C. Update on systemic therapy for advanced soft-tissue sarcoma. Curr Oncol 2020;27:25‐33.
Colin GC, Symons R, Dymarkowski S, Gerber B, Bogaert J. Value of CMR to differentiate cardiac angiosarcoma from cardiac lymphoma. JACC Cardiovasc Imaging 2015;8:744‐6.
Raman SV, Markl M, Patel AR, Bryant J, Allen BD, Plein S, et al. 30-Minute CMR for common clinical indications: A Society for Cardiovascular Magnetic Resonance white paper. J Cardiovasc Magn Reson 2022;24:13.
Acknowledgments
This work was supported by the fund from the National Natural Science Foundation of China (81971645) and Guangdong Provincial People's Hospital (KY0120211130).
Author contribution
LJ, XW, HY, and JQ designed the study. Data collection was performed by HY, JQ, and XW, while data curation was performed by HY, QJ, XW, and FZ. Data analysis was performed by HY and LWCC, of which LWCC is the certified statistician who suggested and supervised all statistical analyses utilized in this study. The manuscript was written and edited by HY, LJ, and KWHC. All authors read and approved the final manuscript.
Disclosures
Hui Yuan, Jia Qiu, Keith W. H. Chiu, Lawrence W. C. Chan, Fen Zhang, Xiaojuan Wei, and Lei Jiang declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were approved by the Ethics Committee at Guangdong Provincial People's Hospital, and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
All editorial decisions for this article, including selection of reviewers and the final decision, were made by guest editor Ahmed Tawakol, MD.
The authors of this article have provided a PowerPoint file, available for download at SpringerLink, which summarises the contents of the paper and is free for re-use at meetings and presentations. Search for the article DOI on SpringerLink.com.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Yuan, H., Qiu, J., Chiu, K.W.H. et al. PET/CT morphology and cardiac conduction disorders help discriminate primary cardiac lymphoma from primary cardiac sarcoma. J. Nucl. Cardiol. 29, 2866–2877 (2022). https://doi.org/10.1007/s12350-022-03042-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-022-03042-0