
Abstract
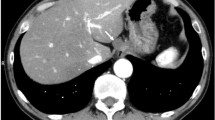
An 81-year-old woman who underwent laparoscopic-assisted low anterior resection with instrumented anastomosis using the double stapling technique for rectal cancer 5 years ago was found to have an enlarged anastomotic mass on computed tomography. On colonoscopy, the anastomotic mass was observed as a 30-mm-sized subepithelial lesion, which was presumed to be the submucosa on endoscopic ultrasonography (EUS). EUS-guided fine-needle aspiration was performed; however, no cellular components were collected. Therefore, endoscopic submucosal dissection (ESD) was performed to remove the entire anastomotic mass. However, any lesion in the submucosa was not detected during ESD, and the lesion was suspected to be located deeper than the submucosa. Therefore, EUS was performed from the muscule layer just below the dissected submucosa, and the mass was detected outside the muscle layer in contact with the rectal wall. Upon endoscopic incision of the muscle layer, milky white mucus was excreted into the rectal lumen. Subsequently, the scope was advanced to an area outside the muscle layer where the mass was located, which was a closed lumen with mucus retention. Surface biopsy of the closed lumen revealed normal colonic mucosa. Therefore, the subepithelial lesion was diagnosed as an implantation cyst arising outside the rectal wall.







Similar content being viewed by others


References
Dukes CE. Submucous implantation cyst of the rectum. Proc R Soc Med. 1929;22:715–8.
Suzuki T, Takashi H, Miyake N, et al. A case of implantation cyst diagnosed by pathologic examination of a specimen obtained by endosocopic mucosal cutting. Gastroenterol Endosc. 2018;60:2512–8.
Katsumata K, Mori Y, Kawakita H, et al. A study of the incidence of implantation cyst at anastomotic sites after low anterior resection of the rectum with the double stapling technique. Langenbecks Arch Surg. 2010;395:465–9.
Fujita Y, Itatani Y, Kawada K, et al. Total pelvic exenteration for mucinous adenocarcinoma arising from an implantation cyst 26 years after surgery for rectal cancer. Asian J Endosc Surg. 2023;16:558–62.
Honda K, Akahoshi K, Matsui N, et al. Role of EUS and EUS guided FNA in the diagnosis of rectal implantation cyst at an anastomosis site after a previous low anterior resection for rectal cancer without evidence of cancer recurrence. Gastrointest Endosc. 2008;68:782–5.
Koizumi N, Kokuba Y, Murayama Y, et al. A case of implantation cyst differentiate from recurrence after surgery for rectal cancer. Jpn J Gastroenterol Surg. 2011;44:1632–8.
Takatsu F, Otani H, Okada N, et al. Laparoscopic resection for implantation cyst at anastomotic site after rectal cancer surgery which was difficult to differentiate from local recurrence: a case report. J Jpn Soc Endosc Surg. 2020;25:177–83.
Watanabe A, Fukunari H, Mito M, et al. Implantation cyst at anastomosis after anterior resection of the rectum-a report of five cases. Gan To Kagaku Ryoho. 2019;46:2288–90.
Hikichi T, Irisawa A, Bhutani MS, et al. Endoscopic ultrasound-guided fine-needle aspiration of solid pancreatic masses with rapid on-site cytological evaluation by endosonographers without attendance of cytopathologists. J Gastroenterol. 2009;44:322–8.
Sena FS, Noguira RF, Oliveira Barroso L, et al. Perianastomotic cyst following rectosigmoidectomy due to adenocarcinoma of the proximal rectum: a case report. J Coloproctol. 2020;40:394–7.
Meylemans DVG, Oostenbrug LE, Bakker CM, et al. Endoscopic ultrasound guided versus surgical transrectal drainage of pelvic abscesses. Acta Chir Belg. 2018;118:181–7.
Acknowledgements
The authors would like to thank Dr. Hirofumi Sekino, Department of Radiology and Nuclear Medicine, Fukushima Medical University, for his advice in evaluating MR images. Moreover, the authors would like to express their deep appreciation to all the endoscopy medical staff and ward staff at Fukushima Medical University Hospital for their assistance with the endoscopic procedures and care of this patient.
Author information
Authors and Affiliations
Contributions
Conception, E.K., T.H., and M.H. Methodology, E.K., T.H., and M.H. Formal analysis, E.K. and M.H. investigation, J.N., T.K., T.Y., and W.S. Resource, E.K. and M.H. Data curation, M.K. and Y.H. Writing—original draft preparation, E.K., T.H., and M.H. Writing—review and editing, J.N., T.K., T.Y., W.S., M.K. Y.H. and H.O. Project administration, T.H. and M.H. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kameoka, E., Hikichi, T., Hashimoto, M. et al. Rectal implantation cyst successfully diagnosed using endoscopic myotomy and endoscopic ultrasonography. Clin J Gastroenterol (2024). https://doi.org/10.1007/s12328-024-01968-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12328-024-01968-1