
Abstract
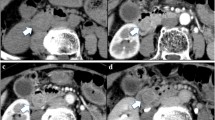
A previously healthy 52-year-old man was referred to our hospital for further evaluation of main pancreatic duct dilatation. The preoperative work-up was consistent with intraductal papillary mucinous carcinoma (IPMC) derived from a mixed type intraductal papillary mucinous neoplasm (IPMN), because multilocular cysts with enhancing thickened pancreatic head walls and dilated pancreatic ducts lined with dysplastic mucinous epithelium, with papillary proliferation from the pancreatic body to the tail, were observed; in addition, the pancreatic juice cytology was class V, which is suggestive of adenocarcinoma. Total pancreatectomy was performed because a definite mass was not found before surgical resection and the tumors could have spread to the tail. The pathological diagnosis was mixed adenoneuroendocrine carcinoma of the pancreatic head. IPMN with high- or low-grade dysplasia was not observed anywhere in the pancreatic duct. The pancreatic ductal adenocarcinoma consisted of large caliber malignant glands with intraluminal flat or papillary structures; therefore, we were unable to recognize a definite pancreatic mass before surgical resection, and suspected an IPMC derived from a mixed type IPMN.






Similar content being viewed by others


References
Cubilla AL, Fitzgerald PJ. Cancer of the exocrine pancreas: the pathologic aspects. CA Cancer J Clin. 1985;35:2–18.
Tanaka M. Pancreatic cancer registry report 2007. J Jpn Pancreas Soc. 2007;22:e1–427 (in Japanese with English abstract).
Chang SM, Yan ST, Wei CK, et al. Solitary concomitant endocrine tumor and ductal adenocarcinoma of pancreas. World J Gastroenterol. 2010;16:2692–7.
Watanabe Y, Okamoto K, Ueno K, et al. A case of mixed adeno-neuroendocrine carcinoma of the pancreas with a ductal cell and large cell type neuroendocrine carcinoma component. J Jpn Pancreas Soc. 2012;27:747–54 (in Japanese with English abstract).
Shibuya K, Kamachi H, Tsuruga Y, et al. A resected case of mixed ductal-neuroendocrine carcinoma of the pancreas. Jpn J Gastroenterol Surg. 2015;48:337–43 (in Japanese with English abstract).
Murata M, Takahashi H, Yamada M, et al. A case of mixed adenoneuroendocrine carcinoma of the pancreas: immunohistochemical analysis for histogenesis. Medicine (Baltimore). 2017;96:e6225.
Yanagisawa A. Invasive carcinoma derived from intraductal papillary neoplasm. J Jpn Pancreas Soc. 2007;22:529–33 (in Japanese with English abstract).
Japan Pancreas Society. General rules for the study of pancreatic cancer. 7th ed. Tokyo: Kanahara Co; 2016.
Sakoda T, Murakami Y, Uemura K, et al. Two cases of mucinous (non-cystic) carcinoma of the pancreas without intraductal papillary mucinous neoplasm. J Jpn Pancreas Soc. 2015;30:600–6 (in Japanese with English abstract).
Suda K, Nobukawa B, Yamasaki S, et al. Pre-existing histological type and developmental mechanism of mucinous noncystic carcinoma of pancreas. Pathol Oncol Res. 2000;6:125–9.
Adsay V, Mino-Kenudson M, Furukawa T, et al. Pathologic evaluation and reporting of intraductal papillary mucinous neoplasms of the pancreas and other tumoral intraepithelial neoplasms of pancreatobiliary tract: recommendations of verona consensus meeting. Ann Surg. 2016;263:162–77.
Luttges J, Zamboni G, Longnecker D, et al. The immunohistochemical mucin expression pattern distinguishes different types of intraductal papillary mucinous neoplasms of the pancreas and determines their relationship to mucinous noncystic carcinoma and ductal adenocarcinoma. Am J Surg Pathol. 2001;25:942–8.
Cho KJ, Kim JY, Lee SS, et al. Mixed acinar-endocrine carcinoma of the pancreas—a case report. J Korean Med Sci. 1996;11:188–92.
Lloyd RV, Osamura RY, Klöppel G, et al. WHO classification of tumours of endocrine organs. 4th ed. Lyon: IARC; 2017.
Kaji K, Seishima J, Yamato M, et al. Clinical utility of endoscopic ultrasound-guided fine-needle aspiration in mixed adenoneuroendocrine carcinoma with signet-ring cells of the pancreas: a case report and review of the literature. Clin J Gastroenterol. 2016;9:43–8.
Chatelain D, Parc Y, Christin-Maitre S, et al. Mixed ductal-pancreatic polypeptide-cell carcinoma of the pancreas. Histopathology. 2002;41:122–6.
Leteurtre E, Brami F, Kerr-Conte J, et al. Mixed ductal-endocrine carcinoma of the pancreas: a possible pathogenic mechanism for arrhythmogenic right ventricular cardiomyopathy. Arch Pathol Lab Med. 2000;124:284–6.
La Rosa S, Marando A, Sessa F, et al. Mixed adenoneuroendocrine carcinomas (MANECs) of the gastrointestinal tract: an update. Cancers (Basel). 2012;4:11–30.
Kimura T, Miyamoto H, Fukuya A, et al. Neuroendocrine carcinoma of the pancreas with similar genetic alterations to invasive ductal adenocarcinoma. Clin J Gastroenterol. 2016;9:261–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Hideki Mori, Keiji Hanada, Tomoyuki Minami, Shigeki Yano, Motomitsu Fukuhara, Hirotsugu Maruyama, Akinori Shimizu, Naomichi Hirano, Fumiaki Hino, Hironobu Amano, and Shuji Yonehara declare that they have no conflict of interest.
Human rights
All procedures followed have been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
Informed consent was obtained from the patient for being included in this report.
Rights and permissions
About this article

Cite this article
Mori, H., Hanada, K., Minami, T. et al. A case of mixed adenoneuroendocrine carcinoma of the pancreas mimicking intraductal papillary mucinous carcinoma. Clin J Gastroenterol 11, 320–326 (2018). https://doi.org/10.1007/s12328-018-0833-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-018-0833-9