
Abstract
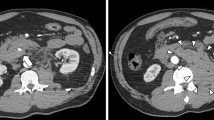
The present study reports a case involving a 17-year-old man who was brought to the emergency department of our hospital with severe upper abdominal pain following a blow received in a rugby game. Emergency computed tomography (CT) revealed severe pancreatic neck injury, and the patient was subsequently given conservative treatment in the High Care Unit. Forty-eight hours later, follow-up enhanced CT revealed that the pancreas was clearly lacerated and the amount of peripancreatic fluid was increasing; furthermore, serum amylase and elastase levels were elevated. Endoscopic retrograde pancreatography revealed that contrast medium in the main pancreatic duct (MPD) had leaked to the parenchyma, indicating an MPD injury. To prevent traumatic pancreatitis from worsening, a stent was inserted endoscopically to a site distal to the injured portion of the MPD. Thereafter, the patient’s condition dramatically improved, and his serum amylase levels returned to normal. CT revealed that the apparent pancreatic edema and peripheral fluid were also decreased. During a short-term follow-up period of 6 months, removal of the stent was uneventfully carried out and the patient did not develop any exocrine or endocrine insufficiency. We suggest that, in some cases, endoscopic management of traumatic pancreatic duct disruption is feasible and effective.




Similar content being viewed by others


References
Leppäniemi A, Haapiainen R, Kiviluoto T, Lempienen M. Pancreatic trauma: acute and late manifestations. Br J Surg. 1988;75:165–7.
Lucas CE. Diagnosis and treatment of pancreatic and duodenal injury. Surg Clin North Am. 1977;57:49–65.
Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Champion HR, Gennarelli TA, et al. Organ injury scaling II: pancreas, duodenum, small bowel, colon, and rectum. J Trauma. 1990;30:1427–9.
Yokota H, Ohizumi A, Kaji M, Kaneko N, Kawashima T, Kitano M et al. Japanese Association for the Surgery of Trauma (JAST). Organ injury classification 2008: pancreatic injury (in Japanese):2008, p 48.
Walker ML. The operative approach to pancreatic injury. J Natl Med Assoc. 1992;84:183–4.
Jurkovich GJ, Carrico CJ. Pancreatic trauma. Surg Clin North Am. 1990;70:575–93.
Yellin AE, Vecchione TR, Donovan AJ. Distal pancreatectomy for pancreatic trauma. Am J Surg. 1972;124:135–42.
Taxier M, Sivak MJ Jr, Coopermann AM, Sullivan BH Jr. Endoscopic retrograde pancreatography in the evaluation of trauma to the pancreas. Surg Gynecol Obstet. 1980;150:65–8.
Lewis G, Krige JEJ, Bornman PC, Terblanche J. Traumatic pancreatic pseudocysts. Br J Surg. 1993;80:89–93.
Bendahan J, Van Rewsburg CJ, Van Vuren B, Muller R. Endoscopic intrapancreatic stent for traumatic duct injury. Injury. 1995;26:553–4.
Huckfeldt R, Agee C, Nicholas WK, Barthel J. Nonoperative treatment of traumatic pancreatic duct disruption using an endoscopically placed stent. J Trauma. 1996;41:143–4.
Kim HS, Lee DK, Kim IW, Baik SK, Kwon SO, Park JW, et al. The role of endoscopc retrograde pancreatography in the treatment of traumatic pancreatic duct injury. Gastrointest Endosc. 2001;54:49–55.
Cay A, Imamoglu M, Bektas O, Ozdemir O, Arslan M, Sarihan H. Nonoperative treatment of traumatic pancreatic duct disruption in children with an endoscopically placed stent. J Pediatr Surg. 2005;40:9–12.
Houben CH, Ade-Ajayi N, Patel S, Kane S, Karani J, Devlin J, et al. Traumatic pancreatic duct injury in children: minimally invasive approach to management. J Pediatr Surg. 2007;42:629–35.
Teh SH, Sheppard BC, Mullins RJ, Schreiber MA, Mayberry JC. Diagnosis and management of blunt pancreatic ductal injury in the era of high-resolution computed axial tomography. Am J Surg. 2007;193:641–3.
Gougeon FW, Legros G, Archambault A, Bessette G, Bastien E. Pancreatic trauma: a new diagnostic approach. Am J Surg. 1976;132:400–2.
Doctor N, Dooley JS, Davidson BR. Assessment of pancreatic duct damage following trauma: is endoscopy retrograde cholangiopancreatography the gold standard? Postgrad Med J. 1995;71:116–7.
Costamagna G, Mutignani M, Ingrosso M, Vamvakousis V, Alevras P, Manta R, et al. Endoscopic treatment of postsurgical external pancreatic fistula. Endoscopy. 2001;33:317–22.
Fulcher AS, Turner MA, Yelon JA, McClain LC, Broderick T, Ivatury RR, et al. Magnetic resonance cholangiopancreatography (MRCP) in the assessment of pancreatic duct trauma and its sequelae: preliminary findings. J Trauma. 2000;48:1001–7.
Gillams AR, Kurzawinski T, Lees WR. Diagnosis of duct disruption and assessment of pancreatic leak with dynamic secretin-stimulated MR cholangiopancreatography. AJR. 2006;186:499–506.
Kozarek RA, Ball TJ, Patterson DJ, Freeny PC, Ryan JA, Traverso LW. Endoscopic transpapillary therapy for disrupted pancreatic duct and peripancreatic fluid collection. Gastroenterology. 1991;100:1362–70.
Kozarek RA. Endoscopic therapy of complete and partial pancreatic duct disruption. Gastrointest Endosc Clin N Am. 1998;8:39–53.
Rerknalmltr R, Sherman S, Fogel EL. Pancreatic duct leak: results of endoscopic management. Gastrointest Endosc 2000; 51:AB139.
Cavallini G, Frulloni L. Somatostatin and octreotide in acute pancreatitis: the never-ending story. Digest Liver Dis. 2001;33:192–201.
Mulligan C, Howell C, Hartley R, Martindale R, Clark J. Conservative management of pancreatic psuedocyst using octreotide acetate. Am Surg. 1995;61:206–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okamoto, H., Hosaka, M., Fujii, H. et al. Successful management of a blunt pancreatic trauma by endoscopic stent placement. Clin J Gastroenterol 3, 204–208 (2010). https://doi.org/10.1007/s12328-010-0161-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-010-0161-1