
Abstract
Introduction
Selective mediastinal lymphadenectomy (SML) and complete mediastinal lymphadenectomy (CML) are two main types of surgery conducted for the treatment of non-small cell lung cancer (NSCLC) plus lobectomy or segmentectomy. It is not known whether stage I NSCLC can benefit from CML. Using the meta-analytical method, our research aimed to find out the worth of SML and CML for the therapy of clinical stage I NSCLC.
Methods
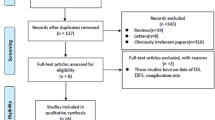
We searched PubMed, Ovid, MEDLINE, Cochrane Controlled Trial Register (CENTRAL), Embase, and Google Scholar for literature published up to June 2021 to evaluate the comparative research and to assess the post-operative complications, overall survival rate, disease-free survival rate, and local and distant recurrence. This meta-analysis was conducted by combining the results of the reported incidences of post-operative complications, local and distant recurrence, and short- and long-term mortality. The pooled odds ratios (OR) and the 95% confidence intervals were calculated by random or fixed effects models to compare the effectiveness between these two methods.
Results
Five retrospective studies and one randomized controlled trial study were included in our research. The six studies included a total of 5713 patients, of whom 1480 were assigned to the SML group and 4233 were assigned to the CML group. No statistically significant differences were found in the 1- and 5-year overall survival rates or the 1-, 3-, and 5-year disease-free survival rates between the two groups. However, the 3-year overall survival favored the SML group (P < 0.05). There were also no statistically significant differences between the local and distant metastasis. Among the postoperative complications, pneumonia, atelectasis, and prolonged air leak were more common in the CML group (P < 0.05). There were no differences in the prevalence of dysrhythmia, chylothorax, acute respiratory distress syndrome, or recurrent laryngeal nerve injury between the two groups, which may be due to the limited sample size.
Conclusion
Considering the comparable survival rates, disease control, and fewer postoperative complications in the evaluated participants, SML is the preferred treatment with less invasiveness for clinical stage I NSCLC.






Similar content being viewed by others


References
Miller KD, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69:363–85. https://doi.org/10.3322/caac.21565.
Herbst RS, Heymach JV, Lippman SM. Lung cancer. N Engl J Med. 2008;359:1367–80. https://doi.org/10.1056/NEJMra0802714.
Meng D, et al. Lymphadenectomy for clinical early-stage non-small-cell lung cancer: a systematic review and meta-analysis. Eur J Cardio-Thorac Surg. 2016;50:597–604. https://doi.org/10.1093/ejcts/ezw083.
Ray MA, Smeltzer MP, Faris NR, Osarogiagbon RU. Survival after mediastinal node dissection, systematic sampling, or neither for early stage NSCLC. J Thorac Oncol. 2020;15:1670–81. https://doi.org/10.1016/j.jtho.2020.06.009.
Abughararah TZ, et al. Lobe-specific lymph node dissection in stage IA non-small-cell lung cancer: a retrospective cohort study. Eur J Cardio-Yhorac Surg. 2021;59:783–90. https://doi.org/10.1093/ejcts/ezaa369.
Shapiro M, et al. Lobe-specific mediastinal nodal dissection is sufficient during lobectomy by video-assisted thoracic surgery or thoracotomy for early-stage lung cancer. Chest. 2013;144:1615–21. https://doi.org/10.1378/chest.12-3069.
Zhao Y, et al. Lobe-specific lymph node dissection in clinical stage IA solid-dominant non-small-cell lung cancer: a propensity score matching study. Clin Lung Cancer. 2021;22:e201–10. https://doi.org/10.1016/j.cllc.2020.09.012.
Maniwa T, et al. Recurrence of mediastinal node cancer after lobe-specific systematic nodal dissection for non-small-cell lung cancer. Eur J Cardio-Thorac Surg. 2013;44:e59-64. https://doi.org/10.1093/ejcts/ezt195.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–84. https://doi.org/10.1136/jech.52.6.377.
Dong S, et al. Systematic mediastinal lymphadenectomy or mediastinal lymph node sampling in patients with pathological stage I NSCLC: a meta-analysis. World J Surg. 2015;39:410–6. https://doi.org/10.1007/s00268-014-2804-8.
Liberati A, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339: b2700. https://doi.org/10.1136/bmj.b2700.
Okada M, et al. Selective mediastinal lymphadenectomy for clinico-surgical stage I non-small cell lung cancer. Ann Thorac Surg. 2006;81:1028–32. https://doi.org/10.1016/j.athoracsur.2005.09.078.
Chen J, Mao F, Song Z, Shen-Tu Y. Retrospective study on lobe-specific lymph node dissection for patients with early-stage non-small cell lung cancer. Zhongguo Fei Ai Za Zhi. 2012;15:531–8. https://doi.org/10.3779/j.issn.1009-3419.2012.09.05.
Jiang W, Chen X, Xi J, Wang Q. Selective mediastinal lymphadenectomy without intraoperative frozen section examinations for clinical stage I non-small-cell lung cancer: retrospective study of 403 cases. World J Surg. 2013;37:392–7. https://doi.org/10.1007/s00268-012-1849-9.
Ma W, Zhang ZJ, Li Y, Ma GY, Zhang L. Comparison of lobe-specific mediastinal lymphadenectomy versus systematic mediastinal lymphadenectomy for clinical stage T1a N0 M0 non-small cell lung cancer. J Cancer Res Ther. 2013;9(Suppl 2):S101-105. https://doi.org/10.4103/0973-1482.119119.
Hishida T, et al. Lobe-specific nodal dissection for clinical stage I and II NSCLC: Japanese multi-institutional retrospective study using a propensity score analysis. J Thorac Oncol. 2016;11:1529–37. https://doi.org/10.1016/j.jtho.2016.05.014.
Patz EF Jr, et al. Lung cancer incidence and mortality in National Lung Screening Trial participants who underwent low-dose CT prevalence screening: a retrospective cohort analysis of a randomised, multicentre, diagnostic screening trial. Lancet Oncol. 2016;17:590–9. https://doi.org/10.1016/s1470-2045(15)00621-x.
Asamura H, Nakayama H, Kondo H, Tsuchiya R, Naruke T. Lobe-specific extent of systematic lymph node dissection for non-small cell lung carcinomas according to a retrospective study of metastasis and prognosis. J Thorac Cardiovasc Surg. 1999;117:1102–11. https://doi.org/10.1016/s0022-5223(99)70246-1.
Han H, Chen H. Selective lymph node dissection in early-stage non-small cell lung cancer. J Thorac Dis. 2017;9:2102–7. https://doi.org/10.21037/jtd.2017.06.04.
Ishiguro F, et al. Effect of selective lymph node dissection based on patterns of lobe-specific lymph node metastases on patient outcome in patients with resectable non-small cell lung cancer: a large-scale retrospective cohort study applying a propensity score. J Thorac Cardiovasc Surg. 2010;139:1001–6. https://doi.org/10.1016/j.jtcvs.2009.07.024.
Howington JA, Blum MG, Chang AC, Balekian AA, Murthy SC. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e278S-e313S. https://doi.org/10.1378/chest.12-2359.
Deng HY, et al. Surgical choice for clinical stage IA non-small cell lung cancer: view from regional lymph node metastasis. Ann Thorac Surg. 2020;109:1079–85. https://doi.org/10.1016/j.athoracsur.2019.10.056.
Hishida T, et al. A randomized Phase III trial of lobe-specific vs systematic nodal dissection for clinical Stage I-II non-small cell lung cancer (JCOG1413). Jpn J Clin Oncol. 2018;48:190–4. https://doi.org/10.1093/jjco/hyx170.
Acknowledgements
Funding
This research was supported by the National Natural Science Foundation of China (81702242) for data collection. The journal’s Rapid Service fees were funded by the Authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Authorship Contributions
Conceptualization: Siyuan Dong; Methodology: Ji Luo and Shize Yang; Wring: Ji Luo and Shize Yang.
Disclosures
Ji Luo, Shize Yang, and Siyuan Dong all confirm they have nothing to disclose.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Luo, J., Yang, S. & Dong, S. Selective Mediastinal Lymphadenectomy or Complete Mediastinal Lymphadenectomy for Clinical Stage I Non-Small Cell Lung Cancer: A Meta-Analysis. Adv Ther 38, 5671–5683 (2021). https://doi.org/10.1007/s12325-021-01954-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-021-01954-w