
Abstract
Introduction
The purpose of this study was to determine prescribing trends in a specialist glaucoma clinic in the UK. Specifically, the aims were to determine which drugs were prescribed as first-, second-, and third-line treatment, the persistence of first-, second-, and third-line treatment regimens, and the proportion of treatment decisions conforming to the European Glaucoma Society (EGS) guidelines.
Methods
A retrospective, non-interventional, single-center, case-note review was performed on a cohort of consecutive patients presenting to a specialist glaucoma clinic for follow-up. Inclusion criteria for the study were (1) a diagnosis of primary open-angle glaucoma or ocular hypertension, (2) glaucoma management entirely within the unit, and (3) minimum of 2 years of follow-up.
Results
A total of 114 case notes met the inclusion criteria. Mean age was 71 years (range 40–95 years). Mean length of follow-up was 56 months (range 24–180 months). Prostaglandin analogues (PGA) were the most popular first-line treatment in 73% of patients. As second-line treatment, PGA were again the predominant class, prescribed in 87% of cases, whereas beta-blockers (BB) were prescribed in 70% of cases. Carbonic anhydrase inhibitors (CAI) and alpha-2 agonists (AA) were more popular in third-line regimens. Second-line treatment was introduced at a mean of 28.0 months after first-line treatment (range 1–120 months, 95% CI 22.1–33.9 months). Third-line treatment was introduced at a mean of 22.9 months after second-line treatment (range 1–96 months, 95% CI 17.1–28.8 months). Breaches to EGS guidelines were most common for third-line treatment and included duplication of drug classes.
Discussion
There was a clear hierarchy of PGA as first-line, BB as second-line, while CAI and AA were considered third-line choices. First-line choices were generally in line with EGS guidelines. There was a tendency to breach guidelines by escalating treatment in dual steps rather than single steps (especially in third-line treatment). Combination drops were popular. In third-line treatment there was an increased incidence of prescribing errors. This data is important in terms of informing patients of the expected treatment course, to remind clinicians about best practice, and also to guide comparisons of cost-effectiveness with other treatment modalities.








Similar content being viewed by others


References
Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82:844–51.
RNIB. Number of adults and children certified with sight impairment and severe sight impairment in England and Wales: April 2011–March 2012. http://www.rnib.org.uk/aboutus/Research/reports/otherresearch/Pages/sight_loss_statistics_report.aspx. Accessed 7 July 2015.
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–7.
Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120(10):1268–79.
Collaborative Normal Tension Glaucoma Study Group. The effectiveness of intraocular pressure reduction in the treatment of normal tension glaucoma. Am J Ophthalmol. 1998;126:298–505.
The AGIS investigators. The Advanced Glaucoma Intervention Study (AGIS) 7. The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130:429–40.
Wahl J. Results of the Collaborative Initial Glaucoma Treatment Study (CIGTS). Ophthalmologe. 2005;102(3):222–6.
Kass MA, Heuer DK, Higginbotham EJ, et al. The ocular hypertension treatment study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701–13.
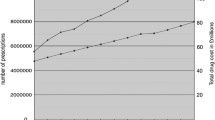
Knox FA, Barry M, McGowan B, O’Brien C. The rising cost of glaucoma drugs in Ireland 1996–2003. Br J Ophthalmol. 2006;90:162–5.
Bateman DN, Clark R, Azuara-Blanco A, Bain M, Forrest J. The effect of new topical treatments on the management of glaucoma in Scotland: an examination of ophthalmological health care. Br J Ophthalmol. 2002;86:551–4.
Macleod SM, Clark R, Forrest J, Bain M, Bateman N, Azuara-Blanco A. A review of glaucoma treatment in Scotland 1994–2004. Eye. 2008;22:251–5.
Connor AJ, Fraser SG. Glaucoma prescribing trends in England 2000 to 2012. Eye. 2014;28:863–9.
Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–7.
EGS. European Glaucoma Society guidelines, 2008. http://www.eugs.org/eng/EGS_guidelines.asp. Accessed 7 July 2015.
Newman-Casey PA, Weizer JS, Heisler M, et al. Systematic review of educational interventions to improve glaucoma medication adherence. Semin Ophthalmol. 2013;28(3):191–201.
Tsai JC. Medication adherence in glaucoma: approaches for optimizing patient compliance. Curr Opin Ophthalmol. 2006;17(2):190–5.
Lin L, Zhao YJ, Chew PT, et al. Comparative efficacy and tolerability of topical prostaglandin analogues for primary open-angle glaucoma and ocular hypertension. Ann Pharmacother. 2014;48(12):1585–93.
Fechtner RD. Prevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medications. Cornea. 2010;29:618–21.
Broadway DC et al. Adverse effects of topical antiglaucoma medication. Arch Ophthalmol. 1994;112:1437–1445.
Khouri AS, Realini T, Fechtner RD. Use of fixed-dose combination drugs for the treatment of glaucoma. Drugs Aging. 2007;24(12):1007–16.
Acknowledgements
No funding or sponsorship was received for this study or publication of this article. The article processing charges were funded by the authors. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published. Glaucoma: Diagnosis and Management. Clinical Guideline (CG85). April 2009 https://www.nice.org.uk/guidance/cg85.
Disclosures
Mark Fajgenbaum and Ejaz Ansari have no disclosures.
Compliance with Ethics Guidelines
The study was approved by a local audit and ethics committee and adhered to the tenets of the Declaration of Helsinki of 1964, as revised in 2013.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/52E8F060264FEC81.
Rights and permissions
About this article

Cite this article
Fajgenbaum, M., Ansari, E. Prescribing Trends in a Glaucoma Clinic and Adherence to EGS Guidelines: A Retrospective, Non-Interventional, Single-Center UK Study. Adv Ther 34, 2033–2042 (2017). https://doi.org/10.1007/s12325-017-0593-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-017-0593-9