
Abstract
Introduction
Crizotinib is recommended as first-line therapy for ALK-positive non-small cell lung cancer (NSCLC), but within a year of treatment initiation many patients develop resistance. With the recent approval of second-generation ALK inhibitors, this study assessed how physicians monitor for and diagnose progression and how they alter treatment following progression on crizotinib.
Methods
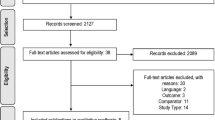
A panel of oncologists from the United States were surveyed regarding their monitoring practices and criteria for diagnosing progression on crizotinib. The physicians also retrospectively provided data (March–June 2016) from the medical charts of their adult patients with locally advanced or metastatic ALK-positive NSCLC who progressed on crizotinib after the approval (April 2014) of the first second-generation ALK inhibitor, ceritinib.
Results
A total of 28 physicians responded to the survey. Data was abstracted on 74 patients. In the physician survey, most physicians (71%) reported monitoring for radiographic progression every 3–4 months. When new lesions were detected, physician response varied. Following a symptomatic isolated lesion, most physicians (75%) would add local therapy and resume crizotinib. Following multiple symptomatic lesions, 96% and 64% of physicians would switch to a new therapy depending on whether the lesions were extracranial or isolated to the brain, respectively. For the patient cohort, physician-defined progression on crizotinib was diagnosed after a median of 10 months, and within 30 days of diagnosis, 86% of patients discontinued crizotinib. Among all patients who discontinued crizotinib, 77% switched to ceritinib, 14% to chemotherapy, and 1% to alectinib. The remaining 7% did not receive additional systemic antineoplastic therapy.
Conclusion
The findings from this physician survey and retrospective chart review study suggest that physician response to the development of new lesions in crizotinib-treated ALK-positive NSCLC patients varies with location and extent of the lesions. Once patients were considered to have progressed, most of them were immediately switched to ceritinib.
Funding
Novartis Pharmaceuticals Corporation.


Similar content being viewed by others


References
Shaw AT, Kim DW, Nakagawa K, et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med. 2013;368(25):2385–94.
Solomon BJ, Mok T, Kim D-W, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371(23):2167–77.
Chun SG, Choe KS, Iyengar P, Yordy JS, Timmerman RD. Isolated central nervous system progression on crizotinib: an achilles heel of non-small cell lung cancer with EML4-ALK translocation? Cancer Biol Ther. 2012;13(14):1376–83.
Sasaki T, Koivunen J, Ogino A, et al. A novel ALK secondary mutation and EGFR signaling cause resistance to ALK kinase inhibitors. Cancer Res. 2011;71(18):6051–60.
Wu J, Savooji J, Liu D. Second- and third-generation ALK inhibitors for non-small cell lung cancer. J Hematol Oncol. 2016;9(1):1–7.
Shaw AT, Solomon B. Anaplastic lymphoma kinase (ALK) fusion oncogene positive non-small cell lung cancer. 2016. http://www.uptodate.com/contents/anaplastic-lymphoma-kinase-alk-fusion-oncogene-positive-non-small-cell-lung-cancer. Accessed Sept 2016.
Peters S. Emerging options after progression during crizotinib therapy. J Clin Oncol. 2016;34(7):643–5.
Costa DB, Shaw AT, Ou SH, et al. Clinical experience with crizotinib in patients with advanced ALK-rearranged non-small-cell lung cancer and brain metastases. J Clin Oncol. 2015;33(17):1881–8.
Solomon BJ, Mok T, Kim DW, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371(23):2167–77.
Ou SH, Janne PA, Bartlett CH, et al. Clinical benefit of continuing ALK inhibition with crizotinib beyond initial disease progression in patients with advanced ALK-positive NSCLC. Ann Oncol. 2014;25(2):415–22.
Food and Drug Administration (FDA). FDA approves ceritinib. 2014. http://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm395386.htm. Accessed Sept 2016.
Food and Drug Administration (FDA). FDA approves new oral therapy to treat ALK-positive lung cancer. 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm476926.htm. Accessed Sept 2016.
Genentech. Alecensa (alectinib) prescribing information. 2015. http://www.gene.com/download/pdf/alecensa_prescribing.pdf. Accessed 13 Oct 2016.
Kim DW, Mehra R, Tan DS, et al. Activity and safety of ceritinib in patients with ALK-rearranged non-small-cell lung cancer (ASCEND-1): updated results from the multicentre, open-label, phase 1 trial. Lancet Oncol. 2016;17(4):452–63.
Tan DS, Araujo A, Zhang J, et al. Comparative efficacy of ceritinib and crizotinib as initial ALK-targeted therapies in previously treated advanced NSCLC: an adjusted comparison with external controls. J Thorac Oncol. 2016;11(9):1550–7.
Crino L, Ahn MJ, De Marinis F, et al. Multicenter phase II study of whole-body and intracranial activity with ceritinib in patients with ALK-rearranged non-small-cell lung cancer previously treated with chemotherapy and crizotinib: results from ASCEND-2. J Clin Oncol. 2016;34(24):2866–73.
National Comprehensive Cancer Network. Non-small cell lung cancer version 4, 2016. www.nccn.org. Accessed 19 Aug 2016.
Guerin A, Sasane M, Wakelee H, et al. Treatment, overall survival, and costs in patients with ALK-positive non-small-cell lung cancer after crizotinib monotherapy. Curr Med Res Opin. 2015;31(8):1587–97.
Cadranel J, Park K, Arrieta O, et al. Characteristics, treatment patterns, and survival among ALK+ non-small cell lung cancer (NSCLC) patients treated with crizotinib: a chart review study. Lung Cancer. 2016;98:9–14.
Chiari R, Metro G, Iacono D, et al. Clinical impact of sequential treatment with ALK-TKIs in patients with advanced ALK-positive non-small cell lung cancer: results of a multicenter analysis. Lung Cancer. 2015;90(2):255–60.
Acknowledgements
This study (LDK 2015-03) and article processing charges were sponsored by Novartis Pharmaceutical Corporation. The sponsor participated in conception and design of the study, analysis and interpretation of data, drafting of the manuscript or revising it critically for important intellectual content, and decision to submit the manuscript for publication. Medical writing assistance was provided by Cinzia Metallo, Ph.D., an employee of Analysis Group, Inc. and funded by Novartis Pharmaceutical Corporation. All authors made substantial contributions to all of the following: conception and design of the study, analysis and interpretation of data, drafting of the manuscript or revising it critically for important intellectual content. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published. A synopsis of the current research was presented in poster format at the IASLC 17th World Conference on Lung Cancer in Vienna, Austria, December 4–7, 2016.
Disclosures
Philip Galebach is an employee of Analysis Group, Inc., a company that has received consulting fees from Novartis Pharmaceuticals Corporation. Iryna Bocharova is an employee of Analysis Group, Inc., a company that has received consulting fees from Novartis Pharmaceuticals Corporation. Rebekah Foster is an employee of Analysis Group, Inc., a company that has received consulting fees from Novartis Pharmaceuticals Corporation. Annie Guerin is an employee of Analysis Group, Inc., a company that has received consulting fees from Novartis Pharmaceuticals Corporation. Alexander R. Macalalad is a former employee of Analysis Group, Inc. Anand A. Dalal is an employee of Novartis Pharmaceuticals Corporation. Kenneth Culver is an employee of Novartis Pharmaceuticals Corporation. Medha Sasane is an employee of Novartis Pharmaceuticals Corporation. Edmond Bendaly has received consultancy fees from Novartis Pharmaceuticals Corporation.
Compliance with Ethics Guidelines
This study did not collect any patient-identifying information and was exempted from review by the Western Institutional Review Board. This article does not contain any new studies with human or animal subjects performed by any of the authors.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to www.medengine.com/Redeem/6E18F06031BB4DC5.
Appendix: Physician Clinical Scenarios and Preferred Course of Action
Appendix: Physician Clinical Scenarios and Preferred Course of Action
A sequence of clinical scenarios will be presented to you. Given the details provided, please indicate your recommendations for the next step in the course of the patient’s treatment. Please note that the treatment received in the scenario might differ from your recommendations and is not meant to reflect current guidelines or standard clinical practice |
Next steps |
a = Continue crizotinib and continue monitoring for new signs of progression |
b = Continue on crizotinib and add local therapy where possible |
c = Switch patient to ceritinib |
d = Switch patient to pemetrexed or another chemotherapy |
e = Switch to supportive care or enroll patient in a clinical trial |
f = Switch patient to alectinib |
Scenario 1 | Scenario 1.1 | Scenario 1.2 | Scenario 1.3 |
|---|---|---|---|
A patient with cough and fatigue was diagnosed with ALK-positive NSCLC and a solitary metastasis in the liver, and the patient was started on crizotinib. After 3 months of therapy, despite excellent adherence to crizotinib, there was little clinical improvement; repeat imaging revealed no change to the existing lesions and no new metastases | The patient was continued on crizotinib for another month and developed progressive headaches and a seizure. Imaging revealed a new brain metastasis in the parietal lobe | The patient was continued on crizotinib for another month, but no local treatment was initiated, and the patient continued to have progressive headaches and seizures. Imaging revealed multiple brain metastases in multiple lobes |
Scenario 2 | Scenario 2.1 | Scenario 2.2 | |
|---|---|---|---|
A different patient diagnosed with ALK-positive NSCLC was started on crizotinib with complete response. After 6 months of therapy, however, the patient developed asthenia and back pain. Imaging revealed a new spinal metastasis at the level of T6 | The patient received radiotherapy and pain control and was continued on crizotinib for another month. The patient’s asthenia improved, and the back pain resolved. However, repeat imaging revealed multiple new lesions in the lung and adrenals |
Rights and permissions
About this article

Cite this article
Bendaly, E., Dalal, A.A., Culver, K. et al. Monitoring for and Characterizing Crizotinib Progression: A Chart Review of ALK-Positive Non-Small Cell Lung Cancer Patients. Adv Ther 34, 1673–1685 (2017). https://doi.org/10.1007/s12325-017-0551-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-017-0551-6