
Abstract
Purpose
To select in a 2-year survey of proximal humerus fractures accessing the emergency department, a population of osteoporotic stable impacted fractures and to randomize them into two groups, one with an immediate intensive mobilization program and the other with an immediate conventional mobilization program.
Methods
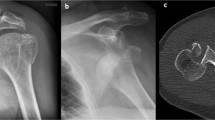
In emergency department, patients with clinical signs of shoulder girdle fracture were submitted to standard X-ray examination and CT scan. Patients with stable (absence of metaphyseal comminution or fifth fragment) osteoporotic (cortical bone thickness lower than 6 mm) impacted (Is any part of metaphysis or head impacted into the shaft? YES/NO) proximal humerus fractures were selected for randomization in one of the two groups. Group 1: early intensive mobilization; Group 2: early conventional mobilization. Functional and radiographic assessment was recorded at 3, 6 and 12 months of follow-up.
Results
In the considered period, 120 patients were affected by a stable impacted osteoporotic proximal humerus fracture. At the final follow-up, 36 patients in group 1 and 39 patients in group 2 were available for statistical analysis. Functional and radiographic scores were comparable, with a trend of significance in favor of group 2. No fracture in any of the group showed significant loss of reduction respect to 6 months of follow-up. 4 (10%) and 1 (2.5%) patients in groups 1 and 2 were not compliant with the rehabilitation program (p = 0.037).
Conclusions
This randomized controlled trial showed that impacted osteoporotic proximal humerus fractures can be managed non-operatively with an early conventional rehabilitation program composed by 10 sessions of passive motion twice a week, followed by recovery of active range of motion for further 10 sessions thrice a week, while no advantage is given by a more aggressive rehabilitation regimen. Self-assisted exercises should be explained to patients to maximize the effects of the assisted program.
Level of evidence
Level 1, randomized controlled double-blinded trial.




Similar content being viewed by others

References
Palvanen M, Kannus P, Niemi S, Parkkari J (2006) Update in the epidemiology of proximal humeral fractures. Clin Orthop Relat Res 442:87–92
Jost B, Spross C, Grehn H, Gerber C (2013) Locking plate fixation of fractures of the proximal humerus: analysis of complications, revision strategies and outcome. J Shoulder Elbow Surg 22:542–549. doi:10.1016/j.jse.2012.06.008
Rangan A, Handoll H, Brealey S, Jefferson L, PROFHER Trial Collaborators et al (2015) Surgical versus nonsurgical treatment of adults with displaced fractures of the proximal humerus the PROFHER randomized clinical trial. JAMA 313:1037–1047. doi:10.1001/jama.2015.1629
Court-Brown CM, Garg A, McQueen MM (2001) The epidemiology of proximal humeral fractures. Acta Orthop Scand 72:365–371
Fjalestad T, Stromsoe K, Blucher J, Tennoe B (2005) Fractures in the proximal humerus: functional outcome and evaluation of 70 patients treated in hospital. Arch Orthop Trauma Surg 125:310–316
Rasmussen S, Hvass I, Dalsgaard J, Christensen S, Holstad E (1992) Displaced proximal humeral fractures: results of conservative treatment. Injury 23:41–43
Lefevre-Colau MM, Babinet A, Fayad F, Fermanian J, Anract P, Roren A, Kansao J, Revel M, Poiraudeau S (2007) Immediate mobilization compared with conventional immobilization for the impacted nonoperatively treated proximal humeral fracture. A randomized controlled trial. J Bone Joint Surg Am 89:2582–2590
Mather J, MacDermid JC, Faber KJ, Athwal GS (2013) Proximal humerus cortical bone thickness correlates with bone mineral density and can clinically rule out osteoporosis. J Shoulder Elbow Surg 22:732–738. doi:10.1016/j.jse.2012.08.018
Hertel R, Hempfing A, Stiehler M, Leunig M (2004) Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg 13:427–433. doi:10.1016/j.jse.2004.01.034
Russo R, Cautiero F, Della Rotonda G (2012) The classification of complex 4-part humeral fractures revisited: the missing fifth fragment and indications for surgery. Musculoskelet Surg 96 Suppl 1:S13–S19. doi:10.1007/s12306-012-0195-2
Constant CR, Murley AHG (1987) A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 214:160–164
Gerber C, Fuchs B, Hodler J (2000) The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am 82:505
Bahrs C, Rolauffs B, Dietz K, Eingartner C, Weise K (2010) Clinical and radiological evaluation of minimally displaced proximal humeral fractures. Arch Orthop Trauma Surg 130:673–679. doi:10.1007/s00402-009-0975-9
Handoll HH, Brorson S (2015) Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev 11(11):CD000434. doi:10.1002/14651858.CD000434.pub4
Hodgson SA, Mawson SJ, Stanley D (2003) Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br 85:419–422
Skedros JG, Mears CS, Burkhead WZ (2017) Ultimate fracture load of cadaver proximal humeri correlates more strongly with mean combined cortical thickness than with areal cortical index, DEXA density, or canal-to-calcar ratio. Bone Joint Res 6:1–7. doi:10.1302/2046-3758.61.BJR-2016-0145.R1
Carbone S, Moroder P, Arceri V, Postacchini R, Gumina S (2014) The amount of humeral head impaction of proximal humeral fractures fixed with the Humerusblock device. Int Orthop 38:1451–1459. doi:10.1007/s00264-014-2327-9
Carbone S, Papalia M (2016) The amount of impaction and loss of reduction in osteoporotic proximal humeral fractures after surgical fixation. Osteoporos Int 27:627–633. doi:10.1007/s00198-015-3304-x
Court-Brown CM, Cattermole H, McQueen MM (2002) Impacted valgus fractures (B1.1) of the proximal humerus. The results of non-operative treatment. J Bone Joint Surg Br 84:504–508
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
IRB: The Health Director of Ospedale San Camillo de Lellis approved this study. Each author certifies that his institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Rights and permissions
About this article

Cite this article
Carbone, S., Razzano, C., Albino, P. et al. Immediate intensive mobilization compared with immediate conventional mobilization for the impacted osteoporotic conservatively treated proximal humeral fracture: a randomized controlled trial. Musculoskelet Surg 101 (Suppl 2), 137–143 (2017). https://doi.org/10.1007/s12306-017-0483-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12306-017-0483-y