
Abstract
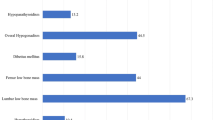
Hemoglobin Eβ-thalassemia is by far the commonest form of thalassemia intermedia. Its phenotype ranges from mild anemia to severe transfusion-dependency necessitating splenectomy in many patients. The present study aimed to systematically analyze both clinical as well as laboratory parameters in profile of Eβ-thalassemia patients after splenectomy in terms of transfusion requirement, infections and other complications. Retrospective study conducted over a period of 3 years included 72 cases of splenectomized Eβ-thalassaemia patients, considering decrease in transfusion requirements, new complications, antibiotic, anti-malarial prophylaxis and iron chelation therapy. Out of 1380 registered Eβ-thalassemia patients, 618 (44.78 %) were regularly transfused and 72(5.22 %) underwent splenectomy. Mean age of diagnosis was 10.3 years. Nineteen patients (26.4 %) underwent splenectomy between 5 and 10 years, 38 cases (52.7 %) between 10 and 20 years. The leading cause (51.39 %) for splenectomy was mechanical discomfort. Mean steady state hemoglobin raised from pre-splenectomy level of 5.43–6.8 gm/dl after splenectomy. Mean transfusion requirement reduced from 18.1 to 7.8 units/year. Mean serum ferritin level increased from 907.58 to 1,091.6 ng/ml. Post-splenectomy; 21 (29.17 %) patients developed facial deformities, 17 (23.6 %) delayed pubertal growth, 11 (15.28 %) venous thromboembolism, five (6.94 %) pulmonary hypertension and four (5.5 %) had extramedullary hematopoiesis. Five (6.96 %) patients had documented bacterial infections and two (2.78 %) suffered from malaria. Forty eight patients (66.67 %) started with iron chelation therapy; but majority (52.7 %) stopped. Major advantage of splenectomy is reduced transfusion requirement, though it cannot prevent skeletal abnormalities and delayed pubertal growth. In resource constraint countries like India, routine anti-malarial and antibacterial prophylaxis is not desirable; iron chelation therapy should be encouraged and ensured.




Similar content being viewed by others


References
Chernoff AI, Minnich V, Nanakorn S et al (1956) Studies on hemoglobin E. I. The clinical, hematologic, and genetic characteristics of the hemoglobin E syndromes. J Lab Clin Med 47:455–489
Chatterjea JB, Swarup S, Ghosh SK et al (1957) Incidence of HbE and of thai trait in Bengalis. Bull Cal Sch Trop Med 5:159–160
Chatterjee JB (1965) Some aspects of HbE and its genetic interaction with thalasemia. Indian J Med Res 53:377–383
Piplani S, Hemoglobin E (2000) Disorders in North East India. JAPI 48:1082–1084
Weatherall DJ (2000) Introduction to the problem of hemoglobin EB thalassemia. J Pediatr Hematol Oncol 22:551
Fucharoen S, Winichagoon P (2000) Clinical and hematologic aspects of hemoglobin E beta-thalassemia. Curr Opin Hematol 7:106–112
Fucharoen S, Ketvichit P, Pootrakul P et al (2000) Clinical manifestation of beta thalassemia/hemoglobin E disease. J Pediatr Hematol Oncol 22:552–557
Hough RE, Kelly R, Nakielny R et al (2003) Extramedullary haemopoiesis in haemoglobin E/beta-thalassaemia. Br J Haematol 120:918
Nadkarni A, Ghosh K, Gorakshaker A et al (1999) Variable clinical severity of Hb E β-thalassemia among Indians. JAPI 47:966–968
Tyagi S, Pari HP, Choudhry VP et al (2004) Clinico-hematological profile of HbE syndrome in adults and children. Hematology 9:57–60
Rees DC, Styles L, Vichinsky EP et al (1998) The hemoglobin E syndromes. Ann NY Acad Sci 850:334–343
Fouladi M, Macmillan ML, Nisbet-Brown E et al (1998) Hemoglobin E/beta thalassemia: Canadian experience. Ann NY Acad Sci 850:410–411
Agarwal S, Gulati R, Singh K (1997) Hemoglobin E-beta thalassemia in Uttar Pradesh. Indian Pediatr 34:287–292
Taher AT, Musallam KM, Cappellini MD et al (2011) Optimal management of b thalassaemia intermedia. Br J Haematol 152:512–523
Panigrahi I, Agarwal S, Gupta T et al (2005) Hemoglobin E-beta Thalassemia: factors affecting phenotype. Indian Pediatr 42:357–362
Giardina P, Forget B (2008) Thalassemia syndromes. In: Hoffman R, Benz E, Shattil S et al (eds) Hematology: basic principles and practice, 5th edn. Churchill Livingstone, Philadelphia, pp 535–563
Gardenghi S, Marongiu MF, Ramos P et al (2007) Ineffective erythropoiesis in beta thalassemia is characterized by increased iron absorption mediated by down regulation of hepcidin and up regulation of ferroportin. Blood 109:5027–5035
Taher A, Ismaeel H, Cappellini MD (2006) Thalassaemia intermedia: revisited. Blood Cells Mol Dis 37:12–20
Olivieri NF, Muraca GM, O’Donnell A et al (2008) Studies in haemoglobin E beta-thalassaemia. Br J Haematol 141:388–397
Tripatara A, Jetsrisuparb A, Teeratakulpisarn J et al (2007) Hemostatic alterations in splenectomized and non-splenectomized patients with beta-thalassemia/hemoglobin E disease. Thromb Res 120:805–810
Eldor A, Rachmilewitz EA (2002) The hypercoagulable state in thalassemia. Blood 99:36–43
Wanachiwanawin W (2000) Infections in E-beta thalassemia. J Pediatr Hematol Oncol 22:581–587
Olivieri NF, De Silva S, Premawardena A et al (2000) Iron overload and iron-chelating therapy in hemoglobin E-beta thalassemia. J Pediatr Hematol Oncol 22:593–597
Conflict of interest
The authors of this paper have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mandal, P.K., Ghosh, M.K. & Bhattacharyya, M. Does Profile of Hemoglobin Eβ-thalassemia Patients Change After Splenectomy? Experience of a Tertiary Thalassemia Care Centre in Eastern India. Indian J Hematol Blood Transfus 31, 446–452 (2015). https://doi.org/10.1007/s12288-014-0498-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12288-014-0498-6