
Abstract
Objectives
(1) To predict pathological complete remission (pCR) and survival after primary systemic therapy (PST) in patients diagnosed with breast cancer by using two different PET/CT based scores: a simplified PERCIST-based PET/CT score (Method 1) and a combined PET/CT score supplemented with the morphological results of the RECIST system (Method 2) and (2) to assess the effect of different breast carcinoma subtypes on tumor response and its evaluation.
Methods
Eighty-eight patients were enrolled in the study who underwent PET/CT imaging before and after PST. PET/CTs were evaluated by changes in maximum Standardized Uptake Value (SUVmax) and tumor size. Method 1 and 2 were applied to predict pathological complete remission (pCR). Kaplan–Meier analyses for survival were performed. Classification into biological subtypes was performed based on the pre-therapeutic tumor characteristics.
Results
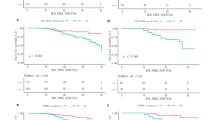
A total of 30/88 patients showed pCR (34.1 %). Comparing pCR/non-pCR patient groups, significant differences were detected by changes in SUVmax (p < 0.001) and tumor size (p < 0.001) regarding the primary breast lesions. To predict pCR, Method 2 had higher sensitivity (72.4 % vs. 44.8 %) and negative predictive value (57.9 % vs. 45.8 %) with lower false negativity rate (16 vs. 32) than Method 1. pCR rate was higher in Her2-positive and triple negative tumors. Despite the significant differences detected between the biological subtypes regarding changes in primary tumor SUVmax (p = 0.007) and size (p = 0.015), the subtypes only had significant impact on response evaluation with Method 2 and not with Method 1. In our study, neither clinical nor pathological CR were predictors of longer progression-free survival.
Conclusions
Our results suggest that combined PET/CT criteria are more predictive of pCR. The effect of biological subtypes is significant on pCR rate as well as on the changes in FDG-uptake and morphological tumor response. Response evaluation with combined criteria was also able to reflect the differences between the biological behavior of breast tumor subtypes.



Similar content being viewed by others


References
Giordano SH. Update on locally advanced breast cancer. Oncologist. 2003;8:521–30.
Kaufmann M, Morrow M, von Minckwitz G, Harris JR. Locoregional treatment of primary breast cancer: consensus recommendations from an International Expert Panel. Cancer. 2010;116:1184–91.
Kinoshita T. Preoperative therapy: recent findings. Breast Cancer. 2011;18:80–4.
Avril N, Sassen S, Roylance R. Response to therapy in breast cancer. J Nucl Med. 2009;50(Suppl 1):55S–63S.
Machiavelli MR, Romero AO, Perez JE, Lacava JA, Dominguez ME, Rodriguez R, et al. Prognostic significance of pathological response of primary tumor and metastatic axillary lymph nodes after neoadjuvant chemotherapy for locally advanced breast carcinoma. Cancer J Sci Am. 1998;4:125–31.
Wolmark N, Wang J, Mamounas E, Bryant J, Fisher B. Preoperative chemotherapy in patients with operable breast cancer: nine-year results from National Surgical Adjuvant Breast and Bowel Project B-18. J Natl Cancer Inst Monogr. 2001; 96–102.
Prowell TM, Pazdur R. Pathological complete response and accelerated drug approval in early breast cancer. N Engl J Med. 2012;366:2438–41.
Tardivon AA, Ollivier L, El Khoury C, Thibault F. Monitoring therapeutic efficacy in breast carcinomas. Eur Radiol. 2006;16:2549–58.
Groheux D, Espie M, Giacchetti S, Hindie E. Performance of FDG PET/CT in the clinical management of breast cancer. Radiology. 2013;266:388–405.
Groheux D, Giacchetti S, Delord M, Hindie E, Vercellino L, Cuvier C, et al. 18F-FDG PET/CT in staging patients with locally advanced or inflammatory breast cancer: comparison to conventional staging. J Nucl Med. 2013;54:5–11.
Wang Y, Zhang C, Liu J, Huang G. Is 18F-FDG PET accurate to predict neoadjuvant therapy response in breast cancer? A meta-analysis. Breast Cancer Res Treat. 2012;131:357–69.
Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: evolving considerations for PET response criteria in solid tumors. J Nucl Med. 2009;50(Suppl 1):122S–50S.
Tőkés T, Szentmártoni Gy, Torgyík L, Kulka J, Lengyel Zs, Györke T, et al. Complexity of the response evaluation during primary systemic therapy of breast cancer. J Clin Oncol ASCO Annual Meeting Abstracts 2014; 32(15_Suppl): e12010.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47.
Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thurlimann B, Senn HJ, et al. Strategies for subtypes—dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011;22:1736–47.
Tokes T, Szentmartoni G, Torgyik L, Kajary K, Lengyel Z, Gyorke T, et al. Response evaluation after primary systemic therapy of Her2 positive breast cancer—an observational cross-sectional study. Croat Med J. 2015;56:128–38.
Lang I, Kahan Z, Pinter T, Dank M, Boer K, Pajkos G, et al. Pharmaceutical therapy of breast cancer. Magy Onkol. 2010;54:237–54.
Pathological Complete Response in Neoadjuvant Treatment of High-Risk Early-Stage Breast Cancer. Use as an endpoint to support accelerated approval. US Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm305501.pdf. 2014 October.
Jones RL, Lakhani SR, Ring AE, Ashley S, Walsh G, Smith IE. Pathological complete response and residual DCIS following neoadjuvant chemotherapy for breast carcinoma. Br J Cancer. 2006;94:358–62.
Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol. 1998;11:155–68.
Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, Cote RJ, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25:118–45.
Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31:3997–4013.
Goldhirsch A, Winer EP, Coates AS, Gelber RD, Piccart-Gebhart M, Thurlimann B, et al. Personalizing the treatment of women with early breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann Oncol. 2013;24:2206–23.
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17:1471–4.
Shankar LK, Hoffman JM, Bacharach S, Graham MM, Karp J, Lammertsma AA, et al. Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute Trials. J Nucl Med. 2006;47:1059–66.
Boellaard R, O’Doherty MJ, Weber WA, Mottaghy FM, Lonsdale MN, Stroobants SG, et al. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: version 1.0. Eur J Nucl Med Mol Imaging. 2010;37:181–200.
Mauri D, Pavlidis N, Ioannidis JP. Neoadjuvant versus adjuvant systemic treatment in breast cancer: a meta-analysis. J Natl Cancer Inst. 2005;97:188–94.
Bonnefoi H, Litiere S, Piccart M, MacGrogan G, Fumoleau P, Brain E, et al. Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: a landmark and two-step approach analyses from the EORTC 10994/BIG 1-00 phase III trial. Ann Oncol. 2014;25:1128–36.
Groheux D, Giacchetti S, Espie M, Rubello D, Moretti JL, Hindie E. Early monitoring of response to neoadjuvant chemotherapy in breast cancer with 18F-FDG PET/CT: defining a clinical aim. Eur J Nucl Med Mol Imaging. 2011;38:419–25.
Keam B, Im SA, Koh Y, Han SW, Oh DY, Cho N, et al. Predictive value of FDG PET/CT for pathologic axillary node involvement after neoadjuvant chemotherapy. Breast Cancer. 2013;20:167–73.
Straver ME, Aukema TS, Olmos RA, Rutgers EJ, Gilhuijs KG, Schot ME, et al. Feasibility of FDG PET/CT to monitor the response of axillary lymph node metastases to neoadjuvant chemotherapy in breast cancer patients. Eur J Nucl Med Mol Imaging. 2010;37:1069–76.
Mghanga FP, Lan X, Bakari KH, Li C, Zhang Y. Fluorine-18 fluorodeoxyglucose positron emission tomography-computed tomography in monitoring the response of breast cancer to neoadjuvant chemotherapy: a meta-analysis. Clin Breast Cancer. 2013;13:271–9.
Groheux D, Hindie E, Giacchetti S, Delord M, Hamy AS, de Roquancourt A, et al. Triple-negative breast cancer: early assessment with 18F-FDG PET/CT during neoadjuvant chemotherapy identifies patients who are unlikely to achieve a pathologic complete response and are at a high risk of early relapse. J Nucl Med. 2012;53:249–54.
Groheux D, Giacchetti S, Hatt M, Marty M, Vercellino L, de Roquancourt A, et al. HER2-overexpressing breast cancer: FDG uptake after two cycles of chemotherapy predicts the outcome of neoadjuvant treatment. Br J Cancer. 2013;109:1157–64.
Humbert O, Cochet A, Riedinger JM, Berriolo-Riedinger A, Arnould L, Coudert B, et al. HER2-positive breast cancer: F-FDG PET for early prediction of response to trastuzumab plus taxane-based neoadjuvant chemotherapy. Eur J Nucl Med Mol Imaging. 2014;41:1525–33.
Jung SY, Kim SK, Nam BH, Min SY, Lee SJ, Park C, et al. Prognostic Impact of [18F] FDG-PET in operable breast cancer treated with neoadjuvant chemotherapy. Ann Surg Oncol. 2010;17:247–53.
Berruti A, Amoroso V, Gallo F, Bertaglia V, Simoncini E, Pedersini R, et al. Pathologic complete response as a potential surrogate for the clinical outcome in patients with breast cancer after neoadjuvant therapy: a meta-regression of 29 randomized prospective studies. J Clin Oncol. 2014;32:3883–91.
Nakajo M, Kajiya Y, Kaneko T, Kaneko Y, Takasaki T, Tani A, et al. FDG PET/CT and diffusion-weighted imaging for breast cancer: prognostic value of maximum standardized uptake values and apparent diffusion coefficient values of the primary lesion. Eur J Nucl Med Mol Imaging. 2010;37:2011–20.
Acknowledgments
The entire research group would like to expresses their gratitude to Mrs. Elvira Rigóné Kálé (Semmelweis University, 2nd Department of Pathology) for her linguistic corrections.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Source of funding
None was involved.
Ethical standards
Ethical approval for the study was given by the Semmelweis University Institutional Review Board. Date and number of the ethical approval: 12 June 2013; TUKEB No. 120/2013. Written informed consent was waived.
About this article

Cite this article
Tőkés, T., Kajáry, K., Szentmártoni, G. et al. Predictive and prognostic value of FDG-PET/CT imaging and different response evaluation criteria after primary systemic therapy of breast cancer. Breast Cancer 24, 137–146 (2017). https://doi.org/10.1007/s12282-016-0685-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-016-0685-4