
Abstract
The roles of aromatase inhibitors (AIs) and luteinizing hormone–releasing hormone (LH–RH) agonists in the management of male breast cancer remain uncertain, with no reports in Japanese men. We report four Japanese male patients with metastatic breast cancer treated with AIs with or without an LH–RH agonist, and consider the relationship between treatment effect and estradiol (E2) concentration. Three patients were initially treated with AI alone after selective estrogen receptor modulators (SERMs), and one received AIs plus an LH–RH agonist after a SERM. Two patients treated with an AI alone responded, one patient with E2 levels below the lower assay limit and the other with levels above the limit. The other treated with an AI alone experienced progression regardless of the E2 levels below the lower assay limit, however, responded after the addition of an LH–RH agonist. E2 concentrations were related to the efficacy of treatment in one patient. The patient initially treated with an AI plus an LH–RH agonist also responded. No grade 3 or 4 adverse events were observed in any of the patients treated with AIs with or without an LH–RH agonist. AIs with or without an LH–RH agonist offer an effective treatment option for hormone receptor-positive metastatic male breast cancer.

Similar content being viewed by others


References
White J, Kearins O, Dodwell D, Horgan K, Hanby AM, Speirs V. Male breast carcinoma: increased awareness needed. Breast Cancer Res. 2011;13(5):219.
Cardoso F, Costa A, Norton L, Cameron D, Cufer T, Fallowfield L, et al. 1st International consensus guidelines for advanced breast cancer (ABC 1). Breast. 2012;21(3):242–52.
NCCN Clinical Practice guideline in Oncology: Breast Cancer. 2014. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp.
Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN. Breast carcinoma in men. Cancer. 2004;101:51–7.
Giordano SH, Buzdar AU, Hortobagyi GN. Breast cancer in men. Ann Intern Med. 2002;137:678–87.
Rushton M, Kwong A, Visram H, Graham N, Petrcich W, Dent S. Treatment outcomes for male breast cancer: a single-center retrospective case control study. Curr Oncol. 2014;21(3):e400–7.
Chavez-Macgregor M, Clarke CA, Lichtensztajn D, Hortobagyi GN, Giordano SH. Male breast cancer according to tumor subtype and race: a population based study. Cancer. 2013;119(9):1611–7.
Eggemann H, Ignatov A, Smith BJ, Altmann U, von Minckwitz G, Röhl FW, et al. Adjuvant therapy with tamoxifen compared to aromatase inhibitors for 257 male breast cancer patients. Breast Cancer Res Treat. 2013;137(2):465–70.
Zumoff B, Fishman J, Cassouto J, Hellman L, Gallagher TF. Estradiol transformation in men with breast cancer. J Clin Endocrinol Metab. 1966;26(9):960–6.
Volm MD. Male breast cancer. Curr Treat Options Oncol. 2003;4(2):159–64.
Harris AL, Dowsett M, Stuart-Harris R, Smith IE. Role of aminoglutethimide in male breast cancer. Br J Cancer. 1986;54(4):657–60.
Mauras N, O’Brien KO, Klein KO, Hayes V. Estrogen suppression in males: metabolic effects. J Clin Endocrinol Metab. 2000;85(7):2370–7.
Doyen J, Italiano A, Largillier R, Ferrero JM, Fontana X, Thyss A. Aromatase inhibition in male breast cancer patients: biological and clinical implications. Ann Oncol. 2010;21(6):1243–5.
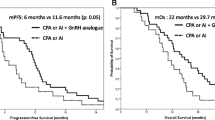
Zagouri F, Sergentanis TN, Koutoulidis V, Sparber C, Steger GG, Dubsky P, et al. Aromatase inhibitors with or without gonadotropin-releasing hotmone analogue in metastatic male breast cancer: a case series. Br J Cancer. 2013;108(11):2259–63.
Di Lauro L, Vici P, Del Medico P, Laudadio L, Tomao S, Giannarelli D, et al. Breast Cancer Res Treat. 2013;141(1):119–23.
Visram H, Kanji F, Dent SF. Endocrine therapy for male breast cancer: rates of toxicity and adherence. Curr Oncol. 2010;17(5):17–21.
Pemmaraju N, Munsell MF, Hortobagyi GN, Giordano SH. Retrospective review of male breast cancer patients: analysis of tamoxifen-related side-effects. Ann Oncol. 2012;23(6):1471–4.
Lash TL, Fox MP, Westrup JL, Fink AK, Silliman RA. Adherence to tamoxifen over the five-year course. Breast Cancer Res Treat. 2006;99(2):215–20.
Hershman DL, Kushi LH, Shao T, Buono D, Kershenbaum A, Tsai WY, et al. Early discontinuation and nonadherence to adjuvant hormonal therapy in a cohort of 8,769 early-stage breast cancer patients. J Clin Oncol. 2010;28(27):4120–8.
Taketani K, Tokunaga E, Yamashita N, Tanaka K, Akiyoshi S, Okada S, et al. Early discontinuation of adjuvant hormone therapy is associated with a poor prognosis in Japanese breast cancer patients. Surg Today. 2014;44(10):1841–6.
Kuba S, Ishida M, Nakamura Y, Taguchi K, Ohno S. Persistence and discontinuation of adjuvant endocrine therapy in women with breast cancer. Breast Cancer 2016;23(1):128–33.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S. Ohno received lecture fees from Chugai and Astrazeneca.
About this article

Cite this article
Kuba, S., Ishida, M., Oikawa, M. et al. Aromatase inhibitors with or without luteinizing hormone–releasing hormone agonist for metastatic male breast cancer: report of four cases and review of the literature. Breast Cancer 23, 945–949 (2016). https://doi.org/10.1007/s12282-016-0679-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-016-0679-2