
Abstract
Background
Abnormal screening mammographic findings are the most common presentation of ductal carcinoma in situ, which usually appears as a cluster of microcalcifications. No report has documented the risk of malignancy between the finding of a cluster of microcalcifications and women with high risk of breast cancer.
Methods
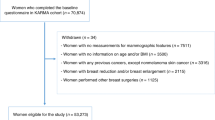
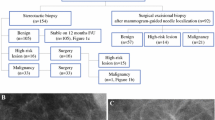
We investigated the morphologic descriptors of a cluster of microcalcifications in women with a high risk for breast cancer and compared the results with the characteristics of a cluster of microcalcifications in other women. A retrospective review was performed for 81 non-palpable clusters of microcalcifications that had stereotactic vacuum-assisted breast biopsy.
Results
The frequency of malignancy associated with a cluster of microcalcifications was 27%. The 50% frequency of malignancy with high risk for breast cancer was higher, but not significantly so, than the 24% frequency of 71 cases without high risk for breast cancer (P = 0.125). The frequency of malignancy and ADH of a cluster of microcalcifications with high risk of breast cancer was 70%, significantly higher than the 30% frequency of 71 cases without high risk of breast cancer (P = 0.028).
Conclusions
A cluster of microcalcifications in women with high risk for breast cancer should be considered suspicious and referred for biopsy.





Similar content being viewed by others

References
Morrow M, Schnitt SJ, Harris JR. Ductal carcinoma in situ and microinvasive carcinoma. In: Harris JR, editor. Disease of the breast. 2nd ed. Philadelphia: Lippincott; 2000. p. 383–401.
Uematsu T, Yuen S, Kasami M, Uchida Y. Dynamic contrast-enhanced MR imaging in screening detected microcalcification lesions of the breast: is there any value? Breast Cancer Res Treat. 2007;103:269–81.
Kettritz U, Morack G, Decker T. Stereotactic vacuum-assisted breast biopsies 500 women with microcalcifications: radiological and pathological correlations. Eur J Radiol. 2005;55:270–6.
Berg WA, Arnoldus CL, Teferra E, Bhargavan M. Biopsy of amorphous breast calcifications: pathologic outcome and yield at stereotactic biopsy. Radiology. 2001;221:495–503.
American College of Radiology. Breast imaging reporting and data system (BI-RADS). 4th ed. Reston: American College of Radiology; 2003.
Burnside ES, Ochsner JE, Fowler KJ, Fine KJ, Salkowski LR, Rubin DL, et al. Use of microcalcification descriptors in BI-RADS 4th edition to stratify risk of malignancy. Radiology. 2007;242:388–95.
Lehman CD, Blume JD, Weatherall P, Thickman, Hylton N, Warner E. Screening women at high risk for breast cancer with mammography and magnetic resonance. Cancer. 2005;103:1898–905.
Sickles EA. Periodic mammographic follow-up of probably benign lesions: results in 3, 184 consecutive cases. Radiology. 1991;179:463–8.
Evans A, Pinder S, Wilson R, Sibbering M, Poller D, Elston C, et al. Ductal carcinoma in situ of the breast: correlation between mammographic and pathologic findings. Am J Roentgenol. 1994;162:1307–11.
Evans A. The diagnosis and management of pre-invasive breast disease: radiological diagnosis. Breast Cancer Res. 2003;5:250–3.
Saslow D, Boetes C, Burke W, Harms S, Leach MO, Lehman CD, et al. American cancer society guidelines for screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75–89.
Liberman L, Abramson AF, Squires FB, Glassman JR, Morris EA, Dershaw DD. The breast imaging reporting and data system: positive predictive value of mammographic features and final assessment categories. Am J Roentgenol. 1998;171:35–40.
D’Orsi CJ. BI-RADS decoded: detailed guidance on potentially confusing issues. Radiol Clin N Am. 2007;45:751–63.
Page DL, Rogers LW. Combined histologic and cytologic criteria for the diagnosis of mammary atypical ductal hyperplasia. Hum Pathol. 1992;23:1095–7.
Tavassoli FA, Norris HJ. A comparison of the results of long-term follow-up for atypical intraductal hyperplasia and intraductal hyperplasia of the breast. Cancer. 1990;65:518–29.
Dershaw D. Does LCIS or ALH without other high-risk lesions diagnosed on core biopsy require surgical excision? Breast J. 2003;9:1–3.
Cohen MA. Cancer upgrades at excisional biopsy after diagnosis of atypical lobular hyperplasia or lobular carcinoma in situ at core-needle biopsy: some reasons why? Radiology. 2004;231:617–21.
Stomper PC, Cholewinski SP, Penetrante RB, Harlos JP, Tsangaris TN. Atypical hyperplasia: frequency and mammographic and pathologic relationships in excisional biopsies guided with mammography and clinical examination. Radiology. 1993;189:667–71.
Page DL, Dupont WD, Rogers LW, Rados MS. Atypical hyperplastic lesions of the female breast. A long-term follow up study. Cancer. 1985;55:2698–708.
Winchester DJ, Bernstein JR, Jeske JM, Nicholson MH, Hahn EA, Goldschmidt RA, et al. Upstaging of atypical ductal hyperplasia after vacuum-assisted 11-gauge stereotactic core needle biopsy. Arch Surg. 2003;138:619–23.
Stomper PC, Connolly JL. Ductal carcinoma in situ of the breast: correlation between mammographic and tumor subtype. Am J Roentgenol. 1992;159:483–5.
Liberman L, Drotman M, Morris EA, LaTrenta LR, Abramson AF, Zakowski MF, et al. Imaging-histologic discordance at percutaneous breast biopsy. Cancer. 2000;89:2538–46.
Foster MC, Helvier MA, Gregory NE, Rebner M, Nees AV, Paramagul C. Lobular carcinoma in situ or atypical lobular hyperplasia at core-needle biopsy: is excisional biopsy necessary? Radiology. 2004;231:813–9.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Uematsu, T., Kasami, M. & Yuen, S. A cluster of microcalcifications: women with high risk for breast cancer versus other women. Breast Cancer 16, 307–314 (2009). https://doi.org/10.1007/s12282-009-0100-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-009-0100-5