
Abstract
Optimization of the atrioventricular (AV) and interventricular (VV) timings of the CRT is the most supposed correctable variable to improve the rate of CRT responder. The aim of the present study has been to evaluate if there is a specific subgroup of patients who can actually benefit the most from a hemodynamic optimization of AV. This is a prospective, observational single-center study that enrolled consecutive patients with clinical indication for CRT; all patients were implanted with CRT-D devices with SonR technology, able to automatically adjust AV and VV delay on a weekly basis. Among 57 patients, 39 (69%) showed a LVESV reduction > 15%. The SonR was able to modify the pacing parameters, but an increase of left atrial diameter was associated to a reduced AV variability, suggesting that an impaired left atrial function could potentially reduce the ability of the SonR algorithm to adjust the correct timing of pacing.

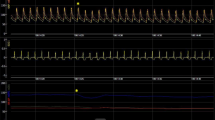
Patients with respectively a high (A) and low (B) AV timing variability, among several parameters that could potentially influence the AV timing, only left atrial dimensions demonstrated a significant impact. In fact an increase of left atrial diameter was associated to a reduced AV variability, suggesting that an impaired left atrial function could potentially reduce the ability of the SonR algorithm to adjust the correct timing of pacing.

Similar content being viewed by others


References
Brignole, M., et al. (2013). 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: The task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European heart rhythm association (EHRA). European Heart Journal, 34, 2281–2329.
Abraham, W. T., et al. (2002). Cardiac resynchronization in chronic heart failure. The New England Journal of Medicine, 346, 1845–1853.
Bristow, M. R., et al. (2004). Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. The New England Journal of Medicine, 350, 2140–2150.
van Bommel, R. J., et al. (2009). Characteristics of heart failure patients associated with good and poor response to cardiac resynchronization therapy: A PROSPECT (predictors of response to CRT) sub-analysis. European Heart Journal, 30, 2470–2477.
Chung, E. S., et al. (2008). Results of the predictors of response to CRT (PROSPECT) trial. Circulation, 117, 2608–2616.
Auricchio, A., & Prinzen, F. W. (2011). Non-responders to cardiac resynchronization therapy: The magnitude of the problem and the issues. Circulation Journal, 75, 521–527.
Mullens, W., et al. (2009). Insights from a cardiac resynchronization optimization clinic as part of a heart failure disease management program. Journal of the American College of Cardiology, 53, 765–773.
Auricchio, A., et al. (2002). Cardiac resynchronization therapy restores optimal atrioventricular mechanical timing in heart failure patients with ventricular conduction delay. Journal of the American College of Cardiology, 39, 1163–1169.
Auricchio, A., et al. (1999). Effect of pacing chamber and atrioventricular delay on acute systolic function of paced patients with congestive heart failure. The Pacing Therapies for Congestive Heart Failure Study Group. The Guidant Congestive Heart Failure Research Group. Circulation, 99, 2993–3001.
Ellenbogen, K. A., et al. (2010). Primary results from the SmartDelay determined AV optimization: A comparison to other AV delay methods used in cardiac resynchronization therapy (SMART-AV) trial: A randomized trial comparing empirical, echocardiography-guided, and algorithmic atrioventricular delay programming in cardiac resynchronization therapy. Circulation, 122, 2660–2668.
Martin, D. O., et al. (2012). Investigation of a novel algorithm for synchronized left-ventricular pacing and ambulatory optimization of cardiac resynchronization therapy: Results of the adaptive CRT trial. Heart Rhythm, 9, 1807–1814.
Abraham, W. T., et al. (2010). Rationale and design of a randomized clinical trial to assess the safety and efficacy of frequent optimization of cardiac resynchronization therapy: the Frequent Optimization Study Using the QuickOpt Method (FREEDOM) trial. American Heart Journal, 159, 944–948.e941.
Ritter, P., et al. (2012). A randomized pilot study of optimization of cardiac resynchronization therapy in sinus rhythm patients using a peak endocardial acceleration sensor vs. standard methods. Europace, 14, 1324–1333.
Rickards, A. F., Bombardini, T., Corbucci, G., & Plicchi, G. (1996). An implantable intracardiac accelerometer for monitoring myocardial contractility. The Multicenter PEA Study Group. Pacing and Clinical Electrophysiology, 19, 2066–2071.
Gorcsan, J., et al. (2008). Echocardiography for cardiac resynchronization therapy: Recommendations for performance and reporting--a report from the American Society of Echocardiography Dyssynchrony writing group endorsed by the Heart Rhythm Society. Journal of the American Society of Echocardiography, 21, 191–213.
Zhang, Q., et al. (2008). The role of repeating optimization of atrioventricular interval during interim and long-term follow-up after cardiac resynchronization therapy. International Journal of Cardiology, 124, 211–217.
Delnoy, P. P., et al. (2013). Association between frequent cardiac resynchronization therapy optimization and long-term clinical response: A post hoc analysis of the clinical evaluation on advanced resynchronization (CLEAR) pilot study. Europace, 15, 1174–1181.
Ponikowski, P., et al. (2016). 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Kardiologia Polska, 74, 1037–1147.
Brugada, J., et al. (2017). Contractility sensor-guided optimization of cardiac resynchronization therapy: Results from the RESPOND-CRT trial. European Heart Journal, 38, 730–738.
Covino, G., et al. (2014). A novel fluoroscopic method of measuring right-to-left interlead distance as a predictor of reverse left ventricular remodeling after cardiac resynchronization therapy. Journal of Interventional Cardiac Electrophysiology, 39, 153–159.
D'Onofrio, A., et al. (2014). Incremental value of larger interventricular conduction time in improving cardiac resynchronization therapy outcome in patients with different QRS duration. Journal of Cardiovascular Electrophysiology, 25, 500–506.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights
All procedures followed were in accordance with ethical standards of the responsible committee on human experimentation and with the Helsinki declaration of 1975, as revisited in 2000.
Informed Consent
Informed consent was obtained from all patients for being included in the study.
Additional information
Associate Editor Sunil Kapur oversaw the review of this article
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Covino, G., Volpicelli, M., Ciardiello, C. et al. Usefulness of Hemodynamic Device-Based Optimization in Heterogeneous Patients Implanted with Cardiac Resynchronization Therapy Defibrillator. J. of Cardiovasc. Trans. Res. 13, 938–943 (2020). https://doi.org/10.1007/s12265-020-10004-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12265-020-10004-9