
Abstract
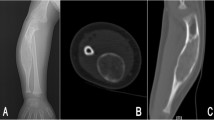
Fibrous dysplasia; is a benign, slow progressive fibroosseous mass of the skeleton, mostly involving the craniofacial joints and long bones. We present a case of monostotic, giant fibrous dysplasia excised by forming a tunnel with two different minimal incisions (tunnel method). A fifty four year-old women was admitted to the outpatient clinic with the complaint of chest pain for the last one month. The postero-anterior chest X-ray revealed a mass lesion that started at the posterior of the right second rib, and extending through the entire rib and causing expansion. Computed tomography of the thorax revealed an 18- 20 cm mass lesion that completely invaded the right second rib, causing expansion of the rib and increased sclerosis, extending to the parietal pleura, compressing the lung parenchyma without deteriorating the integrity of the bone cortex. First, with a high level parascapular incision, the giant mass lesion located in the second rib was separated from the vertebra with safe margins. Later, with an axillary minithoracotomy, by seeing the lesion through the chondral section, the mass lesion was completely excised with intercostal structures and parietal pleura. In the postoperative period, flail chest developed in front of the chest wall was treated with conventional methods. After pathological examination of the specimen, fibrous dysplasia was reported as tumor negative in surgical margins. Although asymptomatic thoracic wall fibrous dysplasia is a benign lesion, surgical resection should not be avoided because of its potential to develop into malignancy.





Similar content being viewed by others


References
Singer FR (1997) Fibrous dysplasia of bone: the bone lesion unmasked. Am J Pathol 151(6):1511–1515
Parekh SG, Donthineni-Rao R, Ricchetti E, Lackman RD (2004) Fibrous dysplasia. The Journal of the American Academy of Orthopaedic Surgeons 12(5):305–313
Snieders MN, Van Kemenade FJ, Van Royen BJ (2009) Monostotic fibrous dysplasia of a lumbar vertebral body with secondary aneurysmal bone cyst formation: a case report. Journal of Medical Case Reports 3:article 7227
Shah ZK, Peh WCG, Koh WL, Shek TWH (2005) Magnetic resonance imaging appearances of fibrous dysplasia. Br J Radiol 78(936):1104–1115
Traibi A, Oueriachi FE, Hammoumi ME, Kabiri EH, Bouzidi AA (2012) Monostotic fibrous dysplasia of the ribs. Interact Cardiovasc Thorac Surg 14:41–43
Matthew R, Di Caprio W, Enneking F (2005) Fibrous dysplasia. Pathophysiology, evaluation and treatment. J Bone Joint Surg Am 87:1848–1864
Kaddour AA, Ben SS, Marghli A et al (2008) Fibrous dysplasia of the rib. Ten case reports. Rev Chir Orthop Reparatrice Appar Mot 94:301–307
Henry A (1969) Monostotic fibrous dysplasia. Journal of Bone and Joint Surgery B 51(2):300–306
Ayadi-Kaddour A, Ben Slama S, Marghli A, Mehouachi R, Djilani H, Kilani T, el Mezni F (2008) Fibrous dysplasia of the rib. Ten case reports. Revue de Chirurgie Orthopedique et Reparatrice de l’Appareil Moteur 94(3):301–307
Hughes EK, James SL, Butt S, Davies AM, Saifuddin A (2006) Benign primary tumours of the ribs. Clin Radiol 61(4):314–322
Remotti F, Feldman F (2012) Nonneoplastic lesions that simulate primary tumors of bone. Archives of Pathology & Laboratory Medicine 136(7):772–788
Tateishi U, Gladish GW, Kusumoto M et al (2003) Chest wall tumors: radiologic findings and pathologic correlation: part 1. Benign tumors. Radiographics 23(6):1477–1490
Terkawi AS, Al-Qahtani KH, Baksh E, Soualmi L, Mohamed AEB, Sabbagh AJ (2011) Fibrous dysplasia and aneurysmal bone cyst of the skull base presenting with blindness: a report of a rare locally aggressive example. Head Neck Oncol 3(1):article 15
Orten SS, Hanna E (1999) Fibrous dysplasia. Biology and indications for surgery. Operat Technig Otoloaryngol Head Neck Surg 10:109–112
Manabu H, Seiichi M, Jun Manabe Taisuke T, Toshio S, Naohiro Izawa Kengo T, Noriyoshi K (2006) Malignant change secondary to fibrous dysplasia. Int J Clin Oncol 11:229–235
Ruggieri P, Sim FH, Bond JR, Unni KK (1994) Malignancies in fibrous dysplasia. Cancer 73:1411–1424
Fitzpatrick KA, Taljanovic MS, Speer DP et al (2004) Imaging findings of fibrous dysplasia with histopathologic and intraoperative correlation. Am J Roentgenol 182(6):1389–1398
Das-Neves-Pereira JC, Bagan P, Coimbra-Israel AP, Grimaillof-Junior A, Cesar-Lopez G, Milanez-de-Campos JR, Riquet M, Biscegli-Jatene F (2009) Fast-track rehabilitation for lung cancer lobectomy: a five-year experience. Eur J Cardiothorac Surg 36:383–391
Loscertales J, Congregado M, Moreno S, Jimenez-Merchan R (2012) Posterolateral thoracotomy without muscle division: a new approach to complex procedures. Interact Cardiovasc Thorac Surg 14:2–4. https://doi.org/10.1093/icvts/ivr059
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hakki, U., Reha, C.M., Mehmet, A. et al. Monostotic Giant Fibrous Dysplasia Excised by Two Different Minimal Incisions (Tunnel Method). Indian J Surg 83, 1542–1546 (2021). https://doi.org/10.1007/s12262-020-02688-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-020-02688-9