
Abstract
Background
Most patients treated for lung cancer experience disease recurrence or progression, resulting in high mortality rates. Computed tomography (CT) is central in evaluating treatment response; however, positron emission tomography (PET) may provide a more rapid and prognostically relevant assessment of changes in disease activity during and after treatment.
Methods
We present a case which illustrates the potential role of PET in assessing treatment response in non-small cell lung cancer (NSCLC) and review the relevant literature.
Results
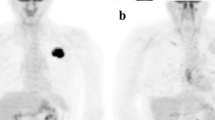
A 49-year-old woman presented with an inoperable pancoast tumour of the lung and was treated with radiochemotherapy (RTCT). PET-CT showed that, while her tumour had not changed in size, the metabolic activity of the tumour had decreased significantly following RTCT. The decision was made to resect the tumour, which was found to contain only a small cluster of viable tumour cells. This case illustrates the clinical relevance of assessing metabolic tumour response in addition to morphologic tumour response. Clinical studies have shown PET to be a valuable addition to treatment response assessments performed using CT in a wide range of clinical situations. Following surgical treatment PET is more effective than CT alone in identifying recurrence, and may be useful in differentiating postoperative scar tissue from active tumour. During systemic treatment, whether with chemotherapy or EGFR-TKIs, the early metabolic response seen in PET can be predictive of the degree of clinical benefit.
Conclusions
In addition to the structural information provided by CT, the metabolic information from PET during or following treatment for NSCLC is increasingly valuable in clinical decision making.



Similar content being viewed by others

References
Vansteenkiste J, Crino L, Dooms C, et al. 2nd ESMO Consensus Conference on Lung Cancer: early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann Oncol. 2014;25:1462–74.
Huber RM, Engel-Riedel W, Kollmeier J, et al. GILT study: oral vinorelbine (NVBo) and cisplatin (P) with concomitant radiotherapy (RT) followed by either consolidation (C) with NVBo plus P plus best supportive care (BSC) or BSC alone in stage (st) III non-small cell lung cancer (NSCLC): final results of a phase (ph) III study. J Clin Oncol. 2012;30. (suppl; abstr 7001).
Rosell R1, Carcereny E, Gervais R, Vergnenegre A. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13(3):239–46
Yang J C-H, Sequist LV, Schuler MH, et al. Overall survival (OS) in patients (pts) with advanced non-small cell lung cancer (NSCLC) harboring common (Del19/L858R) epidermal growth factor receptor mutations (EGFR mut): Pooled analysis of two large open-label phase III studies (LUX-Lung 3 [LL3] and LUX-Lung 6 [LL6]) comparing afatinib with chemotherapy (CT). J Clin Oncol. 2014.(suppl; abstr 8004^).
Jackman DM, Yeap BY, Sequist LV, et al. Exon 19 deletion mutations of epidermal growth factor receptor are associated with prolonged survival in non-small cell lung cancer patients treated with gefitinib or erlotinib. Clin Cancer Res. 2006;12(13):3908–14.
Erasmus JJ, Gladish GW, Broemeling L, et al. Interobserver and intraobserver variability in measurement of non-small-cell carcinoma lung lesions: implications for assessment of tumor response. J Clin Oncol. 2003; 21:2574–82.
Kris MG, Natale RB, Herbst RS, Lynch TJ Jr, Prager D, Belani CP, et al. Efficacy of gefitinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer: a randomized trial. JAMA. 2003;290:2149–58.
Birchard KR, Hoang JK, Herndon JE Jr, Patz EF Jr. Early changes in tumor size in patients treated for advanced stage nonsmall cell lung cancer do not correlate with survival. Cancer. 2009;115:581–6.
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205–16.
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47.
Sohaib A. RECIST rules. Cancer Imaging. 2012;12:345–6.
Young H, Baum R, Cremerius U, et al. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur J Cancer. 1999;35:1773–82.
Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: evolving considerations for PET response criteria in solid tumors. J Nucl Med. 2009;50(Suppl 1):122S–50S.
Ziai D, Wagner T, El Badaoui A, Hitzel A, Woillard JB, Melloni B, et al. Therapy response evaluation with FDG-PET/CT in small cell lung cancer: a prognostic and comparison study of the PERCIST and EORTC criteria. Cancer Imaging. 2013;13:73–80.
Ding Q, Cheng X, Yang L, et al. PET/CT evaluation of response to chemotherapy in non-small cell lung cancer: PET response criteria in solid tumors (PERCIST) versus response evaluation criteria in solid tumors (RECIST). J Thorac Dis. 2014;6:677–83.
Hicks RJ. Role of 18F-FDG PET in assessment of response in non-small cell lung cancer. J Nucl Med. 2009;50(Suppl 1):31S–42S.
Nahmias C, Wahl LM. Reproducibility of standardized uptake value measurements determined by 18F-FDG PET in malignant tumors. J Nucl Med. 2008;49:1804–8.
Weber WA, Ziegler SI, Thodtmann R, Hanauske AR, Schwaiger M. Reproducibility of metabolic measurements in malignant tumors using FDG PET. J Nucl Med. 1999;40:1771–7.
Graham MM, Badawi RD, Wahl RL. Variations in PET/CT methodology for oncologic imaging at U.S. academic medical centers: an imaging response assessment team survey. J Nucl Med. 2011;52:311–7.
Lee P, Weerasuriya DK, Lavori PW, Quon A, Hara W, Maxim PG, et al. Metabolic tumor burden predicts for disease progression and death in lung cancer. Int J Radiat Oncol, Biol, Phys. 2007;69:328–33.
Liao S, Penney BC, Wroblewski K, Zhang H, Simon CA, Kampalath R, et al. Prognostic value of metabolic tumor burden on 18F-FDG PET in nonsurgical patients with non-small cell lung cancer. Eur J Nucl Med Mol Imaging. 2012;39:27–38.
Liao S, Penney BC, Zhang H, Suzuki K, Pu Y. Prognostic value of the quantitative metabolic volumetric measurement on 18F-FDG PET/CT in Stage IV nonsurgical small-cell lung cancer. Acad Radiol. 2012;19:69–77.
Longo DL. Tumor heterogeneity and personalized medicine. N Engl J Med. 2012;366:956–7.
Nishino M, Hatabu H, Johnson BE, McLoud TC. State of the art: response assessment in lung cancer in the era of genomic medicine. Radiology. 2014;271:6–27.
Groome PA, Bolejack V, Crowley JJ, et al. IASLC International Staging Committee, Cancer Research and Biostatistics, Observers to the Committee, Participating Institutions. The IASLC Lung Cancer Staging Project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2(8):694–705.
Backhus LM, Farjah F, Zeliadt SB, et.al. Predictors of imaging surveillance for surgically treated early-stage lung cancer. Ann Thorac Surg. 2014;98(6):1944–52.
Toba H, Sakiyama S, Otsuka H, Kawakami Y, Takizawa H, Kenzaki K, Kondo K, Tangoku A. 18F-fluorodeoxyglucose positron emission tomography/computed tomography is useful in postoperative follow-up of asymptomatic non-small-cell lung cancer patients. Interact Cardiovasc Thorac Surg. 2012;15(5):859–64.
Choi SH, Kim YT, Kim SK, et al. Positron emission tomography-computed tomography for postoperative surveillance in non-small cell lung cancer. Ann Thorac Surg. 2011;92(5):1826–32.
Gorenberg M, Bar-Shalom R, Israel O. Patterns of FDG uptake in post-thoracotomy surgical scars in patients with lung cancer. Br J Radiol. 2008;81(970):821–5.
Lee HY, Lee HJ, Kim YT, Kang CH, Jang BG, Chung DH, Goo JM, Park CM, Lee CH, Kang KW. Value of combined interpretation of computed tomography response and positron emission tomography response for prediction of prognosis after neoadjuvant chemotherapy in non-small cell lung cancer. J Thorac Oncol. 2010;5(4):497–503.
Tanvetyanon T, Eikman EA, Sommers E, Robinson L, Boulware D, Bepler G. Computed tomography response, but not positron emission tomography scan response, predicts survival after neoadjuvant chemotherapy for resectable non-small-cell lung cancer. J Clin Oncol. 2008;26(28):4610–6.
Eschmann SM, Friedel G, Paulsen F, et al. 18F-FDG PET for assessment of therapy response and preoperative re-evaluation after neoadjuvant radio-chemotherapy in stage III non-small cell lung cancer. Eur J Nucl Med Mol Imaging. 2007;34(4):463–71.
Lim HJ, Lee HY, Lee KS, Han J, Kwon OJ, Park K, Ahn YC, Kim BT, Shim YM. Predictive factors for survival in stage IIIA N2 NSCLC patients treated with neoadjuvant CCRT followed by surgery. Cancer Chemother Pharmacol. 2015;75(1):77–85.
Poettgen C, Theegarten D, Eberhardt W, Levegruen S, Gauler T, Krbek T, Stamatis G, Teschler H, Kuehl H, Bockisch A, Stuschke M. Correlation of PET/CT findings and histopathology after neoadjuvant therapy in non-small cell lung cancer. Oncology. 2007;73(5–6):316–23.
Aukema TS, Kappers I, Olmos RA, et al., NEL Study Group. Is 18F-FDG PET/CT useful for the early prediction of histopathologic response to neoadjuvant erlotinib in patients with non-small cell lung cancer? J Nucl Med. 2010;51(9):1344–8.
Schaake EE, Kappers I, Codrington HE, Valdés Olmos RA, Teertstra HJ, van Pel R, Burgers JA, van Tinteren H, Klomp HM. Tumor response and toxicity of neoadjuvant erlotinib in patients with early-stage non-small-cell lung cancer. J Clin Oncol. 2012;30(22):2731–8.
Mac Manus M and Hicks R. The role of positron emission tomography/computed tomography in radiation therapy planning for patients with lung cancer. Semin Nucl Med. 2012;42(5):308–19.
Mac Manus M, Hicks RJ, et al. Positron emission tomography is superior to computed tomography scanning for response-assessment after radical radiotherapy or chemoradiotherapy in patients with non-small cell lung cancer. J Clin Oncol. 2003;21(7):1285–92.
Pöllinger B, Huber RM, Siefert A, Schmid RA, Stratakis D, Dühmke E. The role of positron emission tomography (PET) to determine the response to (chemo-) radiotherapy in locally advanced unresectable lung cancer. Am J Respir Crit Care Med. 2004;169;A753.
Edet-Sanson A., Dubray B, et al. Serial assessment of FDG-PET FDG uptake and functional volume during radiotherapy (RT) in patients with non-small cell lung cancer (NSCLC). Radiother Oncol. 2012;102:251–7.
Mac Manus M., Ding Z, Hogg A, et al. Association between pulmonary uptake of fluorodeoxyglucose detected by positron emission tomography scanning after radiation therapy for non-small-cell lung cancer and radiation pneumonitis. Int J Radiat Oncol Biol Phys. 2011;80(5):1365–71.
Kostakoglu L, Coleman M, Leonard JP, Kuji I, Zoe H, Goldsmith SJ. PET predicts prognosis after 1 cycle of chemotherapy in aggressive lymphoma and Hodgkin’s disease. J Nucl Med. 2002;43:1018–27.
Ott K, Fink U, Becker K, et al. Prediction of response to preoperative chemotherapy in gastric carcinoma by metabolic imaging: results of a prospective trial. J Clin Oncol. 2003;21:4604–10.
Avril N, Sassen S, Schmalfeldt B, et al. Prediction of response to neoadjuvant chemotherapy by sequential F-18-fluorodeoxyglucose positron emission tomography in patients with advanced-stage ovarian cancer. J Clin Oncol. 2005;23:7445–53.
Smith IC, Welch AE, Hutcheon AW, et al. Positron emission tomography using [18F]-fluorodeoxy-D-glucose to predict the pathologic response of breast cancer to primary chemotherapy. J Clin Oncol. 2000;18:1676–88.
Weber WA, Petersen V, Schmidt B, et al. Positron emission tomography in non-small cell lung cancer: prediction of response to chemotherapy by quantitative assessment of glucose use. J Clin Oncol. 2003;21:2651–7.
Hoekstra CJ, Stroobant SG, Smit EF, et al. Prognostic relevance of response evaluation using [18F]-2-fluoro-2-deoxy-D-glucose positron emission tomography in patients with locally advanced non-small-cell lung cancer. J Clin Oncol. 2005;23:8362–70.
Nahmias C., Hanna W.T, et al. Time course of early response to chemotherapy in non-small cell lung cancer patients with 18F-FDG PET/CT. J Nucl Med. 2007;48:744–51
Yang W, Zhang Y, Fu Z, et al. Imaging proliferation of (1)(8)F-FLT PET/CT correlated with the expression of microvessel density of tumour tissue in non-small-cell lung cancer. Eur J Nucl Med Mol Imaging. 2012;39:1289–96.
Su H, Bodenstein C, Dumont R, et al. Monitoring tumor glucose utilization by positron emission tomography for the prediction of treatment response to epidermal growth factor receptor kinase inhibitors. Clin Cancer Res. 2006;12(19):5659–67.
Riely G, Kris MG, Zaho B, et al. Prospective assessment of discontinuation and reinitiation of erlotinib or gefitinib in patients with acquired resistance to erlotinib or gefitinib followed by the addition of everolimus. Clin Cancer Res. 2007;13(17):5150–5.
Benz M, Herrmann K, Walter F, et al. 18F-FDG PET/CT for monitoring treatment responses to the epidermal growth factor receptor inhibitor erlotinib. J Nucl Med. 2011;52(11):1684–9.
Hachemi M, Couturier O, et al. 18F FDG positron emission tomography within two weeks of starting erlotinib therapy can predict response in non-small cell lung cancer patients. PLOS One. 2014;9(2):e87629.
Takahashi R, Hirata H, Tachibana I, et al. Early 18-F-fluorodeoxyglucose positron emission tomography at two days of gefitinib treatment predicts clinical outcome in patients with adenocarcinoma of the lung. Clin Cancer Res. 2012;18(1):220–8.
Kahraman D, Scheffler M, Zander T, et al. Quantitative analysis of response to treatment with erlotinib in advanced non-small cell lung cancer using 18F-FDG and 3-deoxy-3–18F-fluorothymidine PET. J Nucl Med. 2011;52:1871–7.
Mileshkin L, Hicks RJ, Hughes BGM, et al. Changes in 18F-fluorodeoxyglucose and 18-fluorodeoxythymidine positron emission tomography imaging in patients with non-small cell lung cancer treated with erlotinib. Clin Cancer Res. 2011;17(10)3304–15.
Zander T, Scheffler M, Nogova L, et al. Early prediction of nonprogression in advanced non-small cell lung cancer treated with erlotinib by using 18-F fluorodeoxyglucose and 18F fluorothymidine positron emission tomography. J Clin Oncol. 2011;29:1701–8.
Puranik AD, Purandare NC, Shah S, et al. Role of FDG PET/CT in assessing response to targeted therapy in metastatic lung cancers: Morphological versus metabolic criteria. Indian J Nucl Med. 2015;30(1):21–5.
van Gool M.H., Aukema TS, et al. FDG-PET/CT response evaluation during EGFR-TKI treatment in patients with NSCLC. World J Radiol. 2014;6(7):392–8
Tufman AL, Edelmann M, Gamarra F, et al. Preselection based on clinical characteristics in German non-small-cell lung cancer patients screened for EML4-ALK translocation. J Thorac Oncol. 2014;9(1):109–13.
Shaw AT, Kim DW, Nakagawa K, et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med. 2013;368:2385–94.
Gupta SK. Role of Crizotinib in previously treated non-small-cell lung cancer. South Asian J Cancer. 2014;3(2):138–40.
Ou SH I, Bazhenova L, Camidge DR, et al. Rapid and dramatic radiographic and clinical response to an ALK inhibitor (crizotinib, PF02341066) in an ALK translocation-positive patient with non-small cell lung cancer. J Thorac Oncol. 2010;5:2044–6.
Kim SJ, Kim DW, Kim TM, et al. Remarkable tumor response to crizotinib in a 14-year old girl with ALK-positive non-small-cell lung cancer. J Clin Oncol. 2012;30(16):e147–50.
Kerner G, et al. Total body metabolic tumor response in ALK-positive non-small cell lung cancer treated with crizotinib. J Clin Oncol. 2014;32. (suppl; abstr e 19062).
Gambacorti-Passerini C, Messa C, Pogliani EM. Crizotinib in anaplastic large-cell lymphoma. N Engl J Med. 2011;364;8.
Cullinane C, Dorow D, Jackson S, et al. Differential 18F-FDG and 2-deoxz-2-18F-fluorothymidine PET responses to pharmacologic inhibition of the c-MET receptor in preclinical tumor models. J Nucl Med. 2011;52:1261–7.
Camidge DR, Bang Y, Kwak EL, et al. Progression-free survival (PFS) from a phase I study of crizotinib (PF-02341066) in patients with ALK-positive non-small cell lung cancer (NSCLC). J Clin Oncol. 2011;29. (suppl; abstr 2501).
Oxnard GR, Lo P, Jackman DM, et al. Delay of chemotherapy through use of post-progression erlotinib in patients with EGFR-mutant lung cancer. J Clin Oncol. 2012;30(15). (suppl 7547).
Baar J, Silverman P, Lyons J, et al. A vasculature-targeting regimen of preoperative docetaxel with or without bevacizumab for locally advanced breast cancer: impact on angiogenic biomarkers. Clin Cancer Res. 2009;15:3583–90.
Normanno N, Bianco C, De Luca A, Maiello MR, Salomon DS. Target-based agents against ErbB receptors and their ligands: a novel approach to cancer treatment. Endocr Relat Cancer. 2003;10:1–21.
Kim KJ, Li B, Winer J, Armanini M, Gillett N, Phillips HS, et al. Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo. Nature. 1993;362:841–4.
de Langen AJ, van den Boogaart V, Lubberink M, Backes WH, Marcus JT, van Tinteren H, et al. Monitoring response to antiangiogenic therapy in non-small cell lung cancer using imaging markers derived from PET and dynamic contrast-enhanced MRI. J Nucl Med. 2011;52:48–55.
Kurtz DM, Gambhir SS. Tracking cellular and immune therapies in cancer. Advances in cancer research. 2014;124:257–96.
Wolchok JD, Hoos A, O’Day S, et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009;15(23):7412–20.
Sundar R, Soongb R, Chod BC, et al. Immunotherapy in the treatment of non-small cell lung cancer. Lung Cancer. 2014;85(2):101–9.
Oxnard GR, Morris MJ, Hodi FS, Baker LH, Kris MG, Venook AP, et al. When progressive disease does not mean treatment failure: reconsidering the criteria for progression. J Natl Cancer Inst. 2012;104:1534–41.
Brahmer JR, Tykodi SS, Chow LQM, et al. Safety and activity of anti–PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012;366(26):2455–65.
Lynch TJ, Bondarenko I, Luft A, et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non–small-cell lung cancer: results from a randomized, double-blind, multicenter phase II study. J Clin Oncol. 2012. doi:10.1200/JCO.2011.38.4032
Tirkes T, Hollar MA, Tann M, Kohli MD, Akisik F, Sandrasegaran K. Response criteria in oncologic imaging: review of traditional and new criteria. Radiographics. 2013;33:1323–41.
Gilles R, de Geus-Oei LF, Mulders PFA, Oyen WJG. Immunotherapy response evaluation with 18F-FDG-PET in patients with advanced stage renal cell carcinoma. World J Urol. 2013;31:841–6
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tufman, A., Müller-Lisse, U., Reu, S. et al. The relevance of positron emission tomography response in non-small cell lung cancer. memo 8, 119–129 (2015). https://doi.org/10.1007/s12254-015-0213-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12254-015-0213-9