
Abstract
Objectives
To retrospectively investigate the role of 18 F–fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) for the diagnosis and therapeutic response in relapsing polychondritis (RP) patients.
Methods
18F-FDG PET/CT findings were reviewed in six RP patients. The initial scans were performed for all patients, follow-up scans were performed during steroid therapy for five patients. Changes in the abnormal lesions and the maximal standard uptake value (SUVmax) were analyzed.
Results
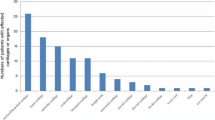
The initial PET/CT scans revealed intense FDG uptake in the cartilages for all six patients. The lesions of abnormal FDG uptake were tracheal/bronchial cartilage (n = 4), costicartilage (n = 4), nasal cartilage (n = 3), cricoid cartilage (n = 3), auricular cartilage (n = 3), arytenoid cartilage (n = 3), thyroid cartilage (n = 2), hyoid cartilage (n = 1) and mediastinum lymph node (n = 1). The mean visual score and the mean SUVmax were 2.96 ± 0.20 and 4.10 ± 0.6. The intense uptake reduced or disappeared during steroid therapy for five patients, the mean visual score and the mean SUVmax were 1.58 ± 1.4 and 1.51 ± 1.4.
Conclusions
18F-FDG PET/CT enables the acquisition of both morphologic and glucose metabolic of the related cartilage structures. It plays a valuable role in assessing almost all cartilage and detecting RP, which is a better selection of a biopsy site as well as therapeutic response monitoring.


Similar content being viewed by others


References
McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine. 1976;55(3):193–215.
Mathew SD, Battafarano DF, Morris MJ. Relapsing polychondritis in the department of defense population and review of the literature. Semin Arthritis Rheum. 2012;42(1):70–83.
Lahmer T, Treiber M, von Werder A, Foerger F, Knopf A, Heemann U, et al. Relapsing polychondritis: an autoimmune disease with many faces. Autoimmun Rev. 2010;9(8):540–6.
Kent PD, Michet CJ, Luthra HS. Relapsing polychondritis. Curr Opin Rheumatol. 2004;16(1):56–61.
Behar JV, Choi YW, Hartman TA, Allen NB, McAdams HP. Relapsing polychondritis affecting the lower respiratory tract. AJR Am J Roentgenol. 2002;178:173–7.
Shi XH, Zhang FC, Chen LB, Ouyang M. The value of 99mTc methylene diphosphonate bone scintigraphy in diagnosing relapsing polychondritis. Chin Med J (Engl). 2006;119(13):1129–32.
Okuyama C, Ushijima Y, Sugihara H, Okitsu S, Ito H, Maeda T. Increased subglottic gallium uptake in relapsing polychondritis. J Nucl Med. 1998;39:1977–9.
Czernin J, Benz MR, Allen-Auerb ach MS. PET/CT imaging: the incremental value of assessing the glucose metabolic phenotype and the structure of cancers in a single examination. Eur J Radiol. 2010;73:470–80.
Sugawara Y, Braun DK, Kison PV, Russo JE, Zasadny KR, Wahl RL. Rapid detection of human infections with fluorine-18 fluorodeoxyglucose and positron emission tomography: preliminary results. Eur J Nucl Med. 1998;25:1238–43.
Signore A, Glaudemans AW. The molecular imaging approach to image infections and inflammation by nuclear medicine techniques. Ann Nucl Med. 2011;25(10):681–700.
Nishiyama Y, Yamamoto Y, Dobashi H, Kameda T, Satoh K, Ohkawa M. [18F]fluorodeoxyglucose positron emission tomography imaging in a case of relapsing polychondritis. J Comput Assist Tomogr. 2007;31:381–3.
De Geeter F, Vandecasleele SJ. Fluorodeoxyglucose PET in relapsing polychondritis. N Engl J Med. 2008;358(5):536–7.
Yokoyama T, Koyama N, Kodama K, Hagiwara K, Kanazawa M. F-fluorodeoxyglucose positron emission tomography for relapsing polychondritis as a diagnostic approach and evaluation of disease activity. BMJ Case Rep. 2009;2009:1591.
Sato M, Hiyama T, Abe T, Ito Y, Yamaguchi S, Uchiumi K, et al. F-18 FDG PET/CT in relapsing polychondritis. Ann Nucl Med. 2010;24:687–90.
Czepczyński R, Guzikowska-Ruszkowska I, Wyszomirska A. Relapsing polychondritis detected in PET/CT. Eur J Nucl Med Mol Imaging. 2012;39(8):1366–7.
Deng H, Chen P, Wang L, Li X, Yi J. Relapsing polychondritis on PET/CT. Clin Nucl Med. 2012;37(7):712–5.
Damiani JM, Levine HL. Relapsing polychondritis–report of ten cases. Laryngoscope. 1979;89(6 Pt 1):929–46.
Roedl JB, Colen RR, King K, Fischman AJ, Mueller PR, Blake MA. Visual PET/CT scoring for nonspecific 18F-FDG uptake in the differentiation of early malignant and benign esophageal lesions. AJR Am J Roentgenol. 2008;191(2):515–21.
Nomori H, Watanabe K, Ohtsuka T, Naruke T, Suemasu K, Uno K. Visual and semiquantitative analyses for F-18 fluorodeoxyglucose PET scanning in pulmonary nodules 1 cm to 3 cm in size. Ann Thorac Surg. 2005;79(3):984–9.
Koyama K, Okamura T, Kawabe J, Nakata B, Chung KH, Ochi H, et al. Diagnostic usefulness of FDG PET for pancreatic mass lesions. Ann Nucl Med. 2001;15(3):217–24.
Tillie-Leblond I, Wallaert B, Leblond D, Salez F, Perez T, Remy-Jardin M, et al. Respiratory involvement in relapsing polychondritis. Clinical, functional, endoscopic, and radiographic evaluations. Medicine (Baltimore). 1998;77(3):168–76.
Faix LE, Branstetter BF 4th. Uncommon CT findings in relapsing polychondritis. AJNR Am J Neuroradiol. 2005;26(8):2134–6.
Diederichs CG, Staib L, Glatting G, Beger HG, Reske SN. FDG PET: elevated plasma glucose reduces both uptake and detection rate of pancreatic malignancies. J Nucl Med. 1998;39:103.
Acknowledgments
The authors would like to thank Yongfeng Luo for his assistance in proof reading of the present manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, J., Li, S., Zeng, Y. et al. 18F-FDG PET/CT is a valuable tool for relapsing polychondritis diagnose and therapeutic response monitoring. Ann Nucl Med 28, 276–284 (2014). https://doi.org/10.1007/s12149-014-0805-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-014-0805-1