
Abstract
Objective
The objective of this study was to evaluate the capability of 11C-methionine (MET)-PET/CT and 18F-2-deoxy-2-fluoro-d-glucose (FDG)-PET/CT to diagnose primary prostate cancer using recently developed Gemini TF PET/CT (Philips Healthcare, Cleveland, OH).
Methods
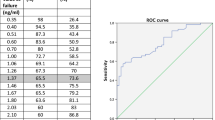
Twenty men who had been referred for a diagnostic work-up for prostate cancer were enrolled in this study. MET- and FDG-PET/CT by high-resolution mode were carried out on the same day prior to prostate biopsy and each maximum standardized uptake value (SUVmax) was compared with the pathological findings. The regions of interest (about 100 mm2 small round) were placed at standard 6 points of the peripheral zone and 4 points in the apex of the transitional zone in cases that had undergone biopsy of the internal gland. We summed two scores if a specimen had inhomogeneous Gleason scores (e.g. GS 7; 4 + 3) and doubled the score when the Gleason score was the same (e.g. GS 8; 4 × 2). We divided the tumors into three groups. If the summed Gleason score of the specimens was 5 or less, they were grouped as NG (no grade with the Gleason score). If the summed Gleason score was 6 or 7, the tumors were defined as LG (low Gleason score group), and if the summed Gleason score was 8, 9 or 10, the tumors were classified as HG (high Gleason score group). The mean SUVmax was calculated and one-way analysis of variance or Kruskal–Wallis test and the Tukey post hoc test were performed for statistical comparisons. The capabilities of MET and FDG for diagnosing prostate cancer were evaluated through analysis of the area under the curve of the receiver operating characteristic (ROC) curve. The cut-off levels of SUVmax for the highest accuracy were determined by the results of the ROC analysis, and the sensitivity, specificity and accuracy were calculated.
Results
The PET images, obtained with Gemini TF PET/CT, allowed visual identification of anatomical locations within the prostate gland. Among the mean SUVmax of MET, FDG early phase and FDG delayed phase, the differences between NG and HG were all statistically significant (P < 0.01). With MET the difference between NG and LG was also significant (P < 0.05). And for the elevation rate from FDG early to delayed phase, the difference between NG and HG was significant (P < 0.05). The cut-off SUVmax, sensitivity, specificity, accuracy for distinguishing between NG and LG + HG by MET, FDG early and delayed phase were 3.15/78.7/75.6/78.3, 2.81/61.7/80.0/70.7 and 3.00/62.8/78.9/70.7, respectively. And the same factors between NG + LG and HG were 3.76/70.1/89.7/82.6, 2.88/70.1/82.9/78.3 and 3.47/62.7/86.3/77.7, respectively.
Conclusions
In terms of the capability to diagnose prostate cancer of high Gleason score (≥8), there was no significant difference between MET and FDG. MET appears to be useful for detecting prostate cancer of both low and high Gleason score.



Similar content being viewed by others

References
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225–49.
Verma S, Rajesh A. A clinically relevant approach to imaging prostate cancer: review. Am J Roentgenol. 2011;196(3 Suppl):S1–10. (quiz S1–4).
Jager GJ, Severens JL, Thornbury JR, de La Rosette JJ, Ruijs SH, Barentsz JO. Prostate cancer staging: should MR imaging be used? A decision analytic approach. Radiology. 2000;215(2):445–51.
Ogura K, Maekawa S, Okubo K, Aoki Y, Okada T, Oda K, et al. Dynamic endorectal magnetic resonance imaging for local staging and detection of neurovascular bundle involvement of prostate cancer: correlation with histopathologic results. Urology. 2001;57(4):721–6.
Hricak H. MR imaging and MR spectroscopic imaging in the pre-treatment evaluation of prostate cancer. Br J Radiol. 2005;78(Spec No 2):S103–11.
Valk PE, Delbeke D, Bailey DL, Townsend DW, Maisey MN. Positron emission tomography. London: Springer; 2006.
Kim EE, Jackson EF. Molecular imaging in oncology. New York: Springer; 1999.
Avril N, Dambha F, Murray I, Shamash J, Powles T, Sahdev A. The clinical advances of fluorine-2-d-deoxyglucose-positron emission tomography/computed tomography in urological cancers. Int J Urol. 2010;17(6):501–11.
Effert PJ, Bares R, Handt S, Wolff JM, Bull U, Jakse G. Metabolic imaging of untreated prostate cancer by positron emission tomography with 18fluorine-labeled deoxyglucose. J Urol. 1996;155(3):994–8.
Hofer C, Laubenbacher C, Block T, Breul J, Hartung R, Schwaiger M. Fluorine-18-fluorodeoxyglucose positron emission tomography is useless for the detection of local recurrence after radical prostatectomy. Eur Urol. 1999;36(1):31–5.
Liu IJ, Zafar MB, Lai YH, Segall GM, Terris MK. Fluorodeoxyglucose positron emission tomography studies in diagnosis and staging of clinically organ-confined prostate cancer. Urology. 2001;57(1):108–11.
Shreve PD, Grossman HB, Gross MD, Wahl RL. Metastatic prostate cancer: initial findings of PET with 2-deoxy-2-[F-18]fluoro-d-glucose. Radiology. 1996;199(3):751–6.
Fanti S, Nanni C, Ambrosini V, Gross MD, Rubello D, Farsad M. PET in genitourinary tract cancers. Q J Nucl Med Mol Imaging. 2007;51(3):260–71.
Fricke E, Machtens S, Hofmann M, van den Hoff J, Bergh S, Brunkhorst T, et al. Positron emission tomography with 11C-acetate and 18F-FDG in prostate cancer patients. Eur J Nucl Med Mol Imaging. 2003;30(4):607–11.
Larson SM, Morris M, Gunther I, Beattie B, Humm JL, Akhurst TA, et al. Tumor localization of 16beta-18F-fluoro-5alpha-dihydrotestosterone versus 18F-FDG in patients with progressive, metastatic prostate cancer. J Nucl Med. 2004;45(3):366–73.
Oyama N, Akino H, Suzuki Y, Kanamaru H, Miwa Y, Tsuka H, et al. Prognostic value of 2-deoxy-2-[F-18]fluoro-d-glucose positron emission tomography imaging for patients with prostate cancer. Mol Imaging Biol. 2002;4(1):99–104.
Lindholm P, Leskinen S, Nagren K, Lehikoinen P, Ruotsalainen U, Teras M, et al. Carbon-11-methionine PET imaging of malignant melanoma. J Nucl Med. 1995;36(10):1806–10.
Lindholm P, Leskinen S, Lapela M. Carbon-11-methionine uptake in squamous cell head and neck cancer. J Nucl Med. 1998;39(8):1393–7.
Miyazawa H, Arai T, Iio M, Hara T. PET imaging of non-small-cell lung carcinoma with carbon-11-methionine: relationship between radioactivity uptake and flow-cytometric parameters. J Nucl Med. 1993;34(11):1886–91.
Kanegae K, Nakano I, Kimura K, Kaji H, Kuge Y, Shiga T, et al. Comparison of MET-PET and FDG-PET for differentiation between benign lesions and lung cancer in pneumoconiosis. Ann Nucl Med. 2007;21(6):331–7.
Dankerl A, Liebisch P, Glatting G, Friesen C, Blumstein NM, Kocot D, et al. Multiple myeloma: molecular imaging with 11C-methionine PET/CT-initial experience. Radiology. 2007;242(2):498–508.
Ogawa T, Shishido F, Kanno I, Inugami A, Fujita H, Murakami M, et al. Cerebral glioma: evaluation with methionine PET. Radiology. 1993;186(1):45–53.
Terakawa Y, Tsuyuguchi N, Iwai Y, Yamanaka K, Higashiyama S, Takami T, et al. Diagnostic accuracy of 11C-methionine PET for differentiation of recurrent brain tumors from radiation necrosis after radiotherapy. J Nucl Med. 2008;49(5):694–9.
Tóth G, Lengyel Z, Balkay L, Salah MA, Trón L, Tóth C. Detection of prostate cancer with 11c-methionine positron emission tomography. J Urol. 2005;173(1):66–9.
Nunez R, Macapinlac HA, Yeung HW, Akhurst T, Cai S, Osman I, et al. Combined 18F-FDG and 11C-methionine PET scans in patients with newly progressive metastatic prostate cancer. J Nucl Med. 2002;43(1):46–55.
Schoder H, Larson S. Positron emission tomography for prostate, bladder, and renal cancer. Semin Nucl Med. 2004;34(4):274–92.
Minamimoto R, Uemura H, Sano F, Terao H, Nagashima Y, Yamanaka S, et al. The potential of FDG-PET/CT for detecting prostate cancer in patients with an elevated serum PSA level. Ann Nucl Med. 2011;25(1):21–7.
Surti S, Kuhn A, Werner ME, Perkins AE, Kolthammer J, Karp JS. Performance of Philips Gemini TF PET/CT scanner with special consideration for its time-of-flight imaging capabilities. J Nucl Med. 2007;48(3):471–80.
Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148(3):839–43.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143(1):29–36.
Watanabe H, Kanematsu M, Kondo H, Kako N, Yamamoto N, Yamada T, et al. Preoperative detection of prostate cancer: a comparison with 11C-choline PET, 18F-fluorodeoxyglucose PET and MR imaging. J Magn Reson Imaging. 2010;31(5):1151–6.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s12149-012-0580-9.
Rights and permissions
About this article
Cite this article
Shiiba, M., Ishihara, K., Kimura, G. et al. Evaluation of primary prostate cancer using 11C-methionine-PET/CT and 18F-FDG-PET/CT. Ann Nucl Med 26, 138–145 (2012). https://doi.org/10.1007/s12149-011-0551-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-011-0551-6