
Abstract
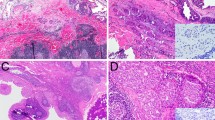
Microsecretory adenocarcinoma (MSA) is a recently described salivary gland tumor with a characteristic histologic and immunophenotypic profile and recurrent MEF2C-SS18 fusions. Because only six cases of MSA have been published, its complete clinicopathologic spectrum is unclear, and its biologic behavior has not been documented. Here, we present an updated and expanded experience of 24 MSA cases. All cases of MSA were obtained from the authors’ files. Immunohistochemistry for S100, SOX10, p63, p40, SMA, calponin, and mammaglobin was performed. Molecular analysis was performed by targeted RNA sequencing, SS18 break apart fluorescence in situ hybridization, and/or reverse transcriptase polymerase chain reaction for MEF2C-SS18 fusion. Clinical follow-up was obtained from medical records. A total of 24 MSA cases were collected, from 13 women and 11 men, ranging from 17 to 83 years (mean 49.5 years). The vast majority (23 of 24) arose in the oral cavity, with the palate (n = 14) and buccal mucosa (n = 6) as the most frequent subsites. Tumors showed consistent histologic features including: (1) microcystic tubules, (2) flattened intercalated duct-like cells, (3) monotonous oval hyperchromatic nuclei, (4) abundant basophilic luminal secretions, (5) fibromyxoid stroma, and (6) circumscribed borders with subtle infiltration. The tumors were very consistently positive for S100 (24 of 24), p63 (24 of 24), and SOX10 (14 of 14) and negative for p40 (0 of 21), calponin (0 of 12) and mammaglobin (0 of 16), while SMA (4 of 20) was variable. MEF2C-SS18 fusion was demonstrated in 21 of 24 cases; in the remaining 3 cases with insufficient RNA, SS18 break apart FISH was positive. Treatment information was available in 17 cases, all of which were managed with surgery only. In 14 cases with follow-up (1–216 months, mean 30), no cases recurred or metastasized. MSA is a distinct salivary gland neoplasm with remarkably consistent clinical, histologic, immunophenotypic, and genetic features that generally behaves in an indolent manner following surgery alone. These observations solidify MSA as a unique, low-grade salivary gland carcinoma that warrants inclusion in the next version of the WHO classification of head and neck tumors.






Similar content being viewed by others


References
Skalova A, Stenman G, Simpson RHW, et al. The role of molecular testing in the differential diagnosis of salivary gland carcinomas. Am J Surg Pathol. 2018;42:e11–27.
Bishop JA, Weinreb I, Swanson D, et al. Microsecretory adenocarcinoma: a novel salivary gland tumor characterized by a recurrent MEF2C-SS18 fusion. Am J Surg Pathol. 2019;43:1023–32.
Kawakami F, Nagao T, Honda Y, et al. Microsecretory adenocarcinoma of the hard palate: a case report of a recently described entity. Pathol Int. 2020;70:781–5.
Bishop JA, Gagan J, Baumhoer D, et al. Sclerosing polycystic "Adenosis" of salivary glands: a neoplasm characterized by PI3K pathway alterations more correctly named sclerosing polycystic adenoma. Head Neck Pathol. 2019.
Agaimy A, Togel L, Haller F, et al. YAP1-NUTM1 gene fusion in porocarcinoma of the external auditory canal. Head Neck Pathol. 2020;14:982–90.
Haas BJ, Dobin A, Li B, et al. Accuracy assessment of fusion transcript detection via read-mapping and de novo fusion transcript assembly-based methods. Genome Biol. 2019;20:213.
Skalova A, Vanecek T, Simpson RHW, et al. Molecular advances in salivary gland pathology and their practical application. Diagn Histopathol. 2012;18:388–96.
Skalova A, Vanecek T, Sima R, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010;34:599–608.
Epivatianos A, Poulopoulos A, Dimitrakopoulos I, et al. Application of α-smooth muscle actin and c-kit in the differential diagnosis of adenoid cystic carcinoma from polymorphous low-grade adenocarcinoma. Oral Oncol. 2007;43:67–76.
Beltran D, Faquin WC, Gallagher G, et al. Selective immunohistochemical comparison of polymorphous low-grade adenocarcinoma and adenoid cystic carcinoma. J Oral Maxillofacial Surg. 2006;64:415–23.
Bishop JA, Koduru P, Veremis BM, et al. SS18 Break-apart fluorescence in situ hybridization is a practical and effective method for diagnosing microsecretory adenocarcinoma of salivary glands. Head Neck Pathol. 2021.
Rashidi A, Fisher SI. FISH-negative, cytogenetically cryptic acute promyelocytic leukemia. Blood Cancer J. 2015;5:e320.
Antonescu CR, Katabi N, Zhang L, et al. EWSR1-ATF1 fusion is a novel and consistent finding in hyalinizing clear-cell carcinoma of salivary gland. Genes Chromosomes Cancer. 2011;50:559–70.
Brayer KJ, Frerich CA, Kang H, et al. Recurrent fusions in MYB and MYBL1 define a common, transcription factor-driven oncogenic pathway in salivary gland adenoid cystic carcinoma. Cancer Discov. 2016;6:176–87.
Dalin MG, Desrichard A, Katabi N, et al. Comprehensive molecular characterization of salivary duct carcinoma reveals actionable targets and similarity to apocrine breast cancer. Clin Cancer Res. 2016;22:4623–33.
Mitani Y, Liu B, Rao PH, et al. Novel MYBL1 gene rearrangements with recurrent MYBL1-NFIB fusions in salivary adenoid cystic carcinomas lacking t(6;9) translocations. Clin Cancer Res. 2016;22:725–33.
Rettig EM, Talbot CC Jr, Sausen M, et al. Whole-genome sequencing of salivary gland adenoid cystic carcinoma. Cancer Prev Res. 2016;9:265–74.
Rooper LM, Mansour M, Yonescu R, et al. The decline of salivary adenocarcinoma not otherwise specified as a tumor entity: reclassification using contemporary immunohistochemical profiling and diagnostic criteria. Am J Surg Pathol. 2020.
Rooper L, Sharma R, Bishop JA. Polymorphous low grade adenocarcinoma has a consistent p63+/p40- immunophenotype that helps distinguish it from adenoid cystic carcinoma and cellular pleomorphic adenoma. Head Neck Pathol. 2015;9:79–84.
Agaimy A, Mueller SK, Bumm K, et al. Intraductal papillary mucinous neoplasms of minor salivary glands with AKT1 p.Glu17Lys mutation. Am J Surg Pathol. 2018;42:1076–82.
Rooper LM, Argyris PP, Thompson LDR, et al. Salivary mucinous adenocarcinoma is a histologically diverse single entity with recurrent AKT1 E17K mutations: clinicopathologic and molecular characterization with proposal for a unified classification. Am J Surg Pathol. 2021.
Ghannoum JE, Freedman PD. Signet-ring cell (mucin-producing) adenocarcinomas of minor salivary glands. Am J Surg Pathol. 2004;28:89–93.
Bastaki JM, Purgina BM, Dacic S, et al. Secretory myoepithelial carcinoma: a histologic and molecular survey and a proposed nomenclature for mucin producing signet ring tumors. Head Neck Pathol. 2014;8:250–60.
Gnepp DR. Mucinous myoepithelioma, a recently described new myoepithelioma variant. Head Neck Pathol. 2013;7(Suppl 1):S85-89.
Funding
This study was funded by the Jane B. and Edwin P. Jenevein M.D Endowment for Pathology at UT Southwestern Medical Center. No external funding was obtained for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that he/she has no conflict of interest as it relates to this research project.
Ethical Approval
All procedures performed in this retrospective data analysis involving human participants were in accordance with the ethical standards of the institutional review board (IRB 112017–073), which did not require informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bishop, J.A., Sajed, D.P., Weinreb, I. et al. Microsecretory Adenocarcinoma of Salivary Glands: An Expanded Series of 24 Cases. Head and Neck Pathol 15, 1192–1201 (2021). https://doi.org/10.1007/s12105-021-01331-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12105-021-01331-7