
Abstract
Objective
To study the Kinetic estimated Glomerular Filtration Rate (KeGFR) using serum creatinine (SCr) for the identification of acute kidney injury (AKI), stages of AKI, and extent of agreement with Kidney Disease Improving Global Outcomes (KDIGO) classification in critically ill children.
Methods
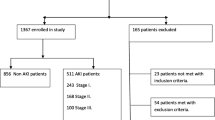
A prospective observational study was conducted in a pediatric intensive care unit (PICU) in a tertiary care institute of South India from July through August 2018. Sixty children were enrolled. The patients with known End-Stage Renal Disease (ESRD), with previous renal transplantation, admission SCr more than 4 mg per dL, expired within 24 h of admission and patients who underwent Renal Replacement Therapy (RRT) before PICU admission were excluded. KeGFR was calculated for the first seven days, and the worst achieved value was determined. AKI staging by KDIGO was compared with AKI by KeGFR value. The requirement of RRT, multi-organ dysfunction syndrome (MODS), mechanical ventilation, cumulative fluid balance, PICU stay, and hospital mortality was recorded.
Results
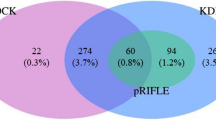
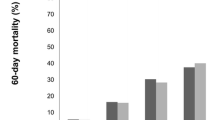
AKI detection by KeGFR method showed a sensitivity of 93% (95% CI 80% - 98.2%) and specificity of 76% (95% CI 49.8% - 92.2%) compared to KDIGO criteria. The good agreement between KDIGO and KeGFR values for AKI was noted (Kappa = 0.71, p < 0.001). It was observed that 81.3% (n = 13) of Group-I, 56% (n = 14) of Group-II, 77.8% (n = 7) of Group-III and 90% (n = 9) of Group-IV by KeGFR were graded as Stage-0, Stage-1, Stage-2 and Stage-3 of AKI by KDIGO criteria respectively (p < 0.001). There was no significant difference noted in secondary outcomes. The survival of children with AKI and those without AKI (by both KDIGO staging and KeGFR) showed no significant difference.
Conclusions
KeGFR is highly sensitive, and there is a good agreement with KDIGO criteria in the identification of AKI in critically ill children. Further research is required to validate these study results.
Similar content being viewed by others
References
Kaddourah A, Basu RK, Bagshaw SM. Goldstein SL; AWARE investigators. Epidemiology of acute kidney injury in critically ill children and young adults. N Engl J Med. 2017;376:11–20.
de Oliveira MF, Oliveira SA, de Lima E, Souza PF, et al. Kinetic estimated glomerular filtration rate in critically ill patients: beyond the acute kidney injury severity classification system. Crit Care. 2017;21:280.
O’Sullivan ED, Doyle A. The clinical utility of kinetic glomerular filtration rate. Clin Kidney J. 2017;10:202–8.
Chen S. Kinetic glomerular filtration rate in routine clinical practice—applications and possibilities. Adv Chronic Kidney Dis. 2018;25:105–14.
Seelhammer TG, Maile MD, Heung M, Haft JW, Jewell ES, Engoren M. Kinetic estimated glomerular filtration rate and acute kidney injury in cardiac surgery patients. J Crit Care. 2016;31:249–54.
Hekmat R, Eshraghi H, Esmailpour M, Hassankhani GG. Kinetic glomerular filtration rate estimation compared with other formulas for evaluating acute kidney injury stage early after kidney donation. Exp Clin Transplant. 2017;15:104–9.
Endre ZH, Pianta TJ, Pickering JW. Timely diagnosis of acute kidney injury using kinetic eGFR and the creatinine excretion to production ratio, E/eG-creatinine can be useful! Nephron. 2016;132:312–6.
Dewitte A, Joannès-Boyau O, Sidobre C, et al. Kinetic eGFR and novel AKI biomarkers to predict renal recovery. Clin J Am Soc Nephrol. 2015;10:1900–10.
Pianta TJ, Endre ZH, Pickering JW, Buckley NA, Peake PW. Kinetic estimation of GFR improves prediction of dialysis and recovery after kidney transplantation. PLoS One. 2015;10:e0125669.
Stevens LA, Levey AS. Measured GFR as a confirmatory test for estimated GFR. J Am Soc Nephrol. 2009;20:2305–13.
Schwartz GJ, Muñoz A, Schneider MF, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20:629–37.
Heilbron DC, Holliday MA, Al-Dahwi A, Kogan BA. Expressing glomerular filtration rate in children. Pediatr Nephrol. 1991;5:5–11.
Chen S. Retooling the creatinine clearance equation to estimate kinetic GFR when the plasma creatinine is changing acutely. J Am Soc Nephrol. 2013;24:877–88.
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120:c179–84.
Lopes CL, Piva JP. Fluid overload in children undergoing mechanical ventilation. Rev Bras Ter Intensiva. 2017;29:346–53.
World Health Organization. WHO child growth standards and the identification of severe acute malnutrition in infants and children. A Joint Statement. Geneva, Switzerland: WHO; 2009. Available at: https://apps.who.int/iris/bitstream/handle/10665/44129/9789241598163_eng.pdf?ua=1. Accessed 15 Aug 2018.
Bairy M, See FH, Lim RS. Using the kinetic estimating glomerular filtration rate equation for estimating glomerular filtration rate and detecting acute kidney injury: a pilot study. Nephron. 2018;140:231–9.
Acknowledgements
The authors acknowledge the contribution of Mrs. S. Raja Deepa B.Com, MCA (JIPMER Campus, Puducherry, India) for support of data entry in a blinded manner and editing of the manuscript; Mr. Rakesh Mohindra (Punjab University, Chandigarh, India) and Mrs. Thenmozhi M M.Sc, Ph.D. (Senior Demonstrator, CMC, Vellore, India) for helping the statistical analysis and Mrs. Harpreet Kaur (Punjab University, Chandigarh, India), and Mrs. Neelima Chadha (Tulsi Das Library, PGIMER, Chandigarh, India) for helping medical literature search.
Author information
Authors and Affiliations
Contributions
RR was involved in the management of the patients. AVL collected the data, reviewed the literature and drafted the first manuscript. RB and TR contributed to protocol development, statistical analysis and first draft manuscript. RR conceptualized the study, reviewed the literature and critically reviewed the manuscript. All authors approved the final version of the manuscript. RR is the guarantor of the paper.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Source of Funding
In support, part, by department and institution.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Latha, A.V., Rameshkumar, R., Bhowmick, R. et al. Kinetic Estimated Glomerular Filtration Rate and Severity of Acute Kidney Injury in Critically Ill Children. Indian J Pediatr 87, 995–1000 (2020). https://doi.org/10.1007/s12098-020-03314-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-020-03314-y