
Abstract
Objective
Improving vancomycin therapy with therapeutic drug monitoring is recommended. Over the past few years, a few studies have demonstrated that trough concentrations may not be the optimal parameter for monitoring vancomycin concentration and Area under the curve (AUC) should be used instead. In this study authors evaluate two methods to estimate the AUC. The first method is based on linear regression using only a trough concentration. The second method uses a simplified two-sample equation-based strategy to estimate the AUC.
Methods
Data from 70 infant patients were collected retrospectively from their medical records at King Saud University Medical City. The prediction accuracy for vancomycin therapy monitoring was optimized by comparing the two methods for the AUC calculation, the simple linear regression and simplified two-sample equation-based strategy.
Results
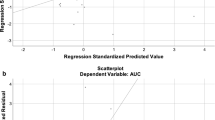
The target AUC > 400 μg × h/ml was achieved in 10%, 71%, and 100% of patients with trough concentration ranges of 5–10, 10–15, and > 15 μg/ml, respectively. There was a strong correlation between the predicted and observed AUC calculated using the simplified two-sample equation-based strategy (R2 = 0.91, bias = −3.9%, precision =12%).
Conclusions
The target AUC > 400 μg × h/ml can be achieved at trough concentrations <15 μg/ml in most patients. Targeting trough concentrations >15 can lead to overdoing and increase risk of nephrotoxicity. The authors recommend estimating the AUC using the simplified two-sample equation strategy for more precise dosing of vancomycin. Using AUC-guided dosing instead of the trough-guided approach can prevent over dosing and reduce the risk of nephrotoxicity.



Similar content being viewed by others


References
Casapao AM, Lodise TP, Davis SL, et al. Association between vancomycin day 1 exposure profile and outcomes among patients with methicillin-resistant Staphylococcus aureus infective endocarditis. Antimicrob Agents Chemother. 2015;59:2978–85.
Lodise TP, Drusano GL, Zasowski E, et al. Vancomycin exposure in patients with methicillin-resistant Staphylococcus aureus bloodstream infections: how much is enough? Clin Infect Dis. 2014;59:666–75.
Moise-Broder PA, Forrest A, Birmingham MC, Schentag JJ. Pharmacodynamics of vancomycin and other antimicrobials in patients with Staphylococcus aureus lower respiratory tract infections. Clin Pharmacokinet. 2004;43:925–42.
Janssen EJ, Välitalo PA, Allegaert K, et al. Towards rational dosing algorithms for vancomycin in neonates and infants based on population pharmacokinetic modeling. Antimicrob Agents Chemother. 2016;60:1013–21.
Marsot A, Boulamery A, Bruguerolle B, Simon N. Vancomycin: a review of population pharmacokinetic analyses. Clin Pharmacokinet. 2012;51:1–13.
Broome L, So TY. An evaluation of initial vancomycin dosing in infants, children, and adolescents. Int J Pediatr. 2011;2011:470364.
Oudin C, Vialet R, Boulamery A, Martin C, Simon N. Vancomycin prescription in neonates and young infants: toward a simplified dosage. Arch Dis Child Fetal Neonatal Ed. 2011;96:F365–70.
Sheng XY, Chen CY, Ma LY, Liu YO, Zhou Y, Cui YM. Population pharmacokinetics of vancomycin in Chinese infants. Int J Clin Pharmacol Ther. 2017;55:558–66.
Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52:e18–55.
Prybylski JP. Vancomycin trough concentration as a predictor of clinical outcomes in patients with Staphylococcus aureus bacteremia: a meta-analysis of observational studies. Pharmacotherapy. 2015;35:889–98.
Frymoyer A, Hersh AL, El-Komy MH, et al. Association between vancomycin trough concentration and area under the concentration-time curve in neonates. Antimicrob Agents Chemother. 2014;58:6454–61.
van Hal SJ, Paterson DL, Lodise TP. Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter. Antimicrob Agents Chemother. 2013;57:734–44.
Lodise TP, Patel N, Lomaestro BM, Rodvold KA, Drusano GL. Relationship between initial vancomycin concentration-time profile and nephrotoxicity among hospitalized patients. Clin Infect Dis. 2009;49:507–14.
Patel K, Crumby AS, Maples HD. Balancing vancomycin efficacy and nephrotoxicity: should we be aiming for trough or AUC/MIC? Paediatr Drugs. 2015;17:97–103.
Seixas GT, Araujo OR, Silva DC, Arduini RG, Petrilli AS. Vancomycin therapeutic targets and nephrotoxicity in critically ill children with cancer. J Pediatr Hematol Oncol. 2016;38:e56–62.
Bosso JA, Nappi J, Rudisill C, et al. Relationship between vancomycin trough concentrations and nephrotoxicity: a prospective multicenter trial. Antimicrob Agents Chemother. 2011;55:5475–9.
Pritchard L, Baker C, Leggett J, Sehdev P, Brown A, Bayley KB. Increasing vancomycin serum trough concentrations and incidence of nephrotoxicity. Am J Med. 2010;123:1143–9.
Bhargava V, Malloy M, Fonseca R. The association between vancomycin trough concentrations and acute kidney injury in the neonatal intensive care unit. BMC Pediatr. 2017;17:50.
McKamy S, Hernandez E, Jahng M, Moriwaki T, Deveikis A, Le J. Incidence and risk factors influencing the development of vancomycin nephrotoxicity in children. J Pediatr. 2011;158:422–6.
Knoderer CA, Nichols KR, Lyon KC, Veverka MM, Wilson AC. Are elevated vancomycin serum trough concentrations achieved within the first 7 days of therapy associated with acute kidney injury in children? J Pediatric Infect Dis Soc. 2014;3:127–31.
Finch NA, Zasowski EJ, Murray KP, et al. The impact of vancomycin area under the concentration-time curve-guided dosing on vancomycin-associated nephrotoxicity: a quasi-experiment. Antimicrob Agents Chemother. 2017;61:e01293–17.
Neely MN, Kato L, Youn G, et al. Prospective trial on the use of trough concentration versus area under the curve to determine therapeutic vancomycin dosing. Antimicrob Agents Chemother. 2018;62:pii: e02042-17.
Le J, Bradley JS, Murray W, et al. Improved vancomycin dosing in children using area under the curve exposure. Pediatr Infect Dis J. 2013;32:e155–63.
Pai MP, Rodvold KA. Aminoglycoside dosing in patients by kidney function and area under the curve: the Sawchuk-Zaske dosing method revisited in the era of obesity. Diagn Microbiol Infect Dis. 2014;78:178–87.
Pai MP, Neely M, Rodvold KA, Lodise TP. Innovative approaches to optimizing the delivery of vancomycin in individual patients. Adv Drug Deliv Rev. 2014;77:50–7.
Pai MP, Russo A, Novelli A, Venditti M, Falcone M. Simplified equations using two concentrations to calculate area under the curve for antimicrobials with concentration-dependent pharmacodynamics: daptomycin as a motivating example. Antimicrob Agents Chemother. 2014;58:3162–7.
Sheiner LB, Beal SL. Some suggestions for measuring predictive performance. J Pharmacokinet Biopharm. 1981;9:503–12.
Ragab AR, Al-Mazroua MK, Al-Harony MA. Incidence and predisposing factors of vancomycin-induced nephrotoxicity in children. Infect Dis Ther. 2013;2:37–46.
Neely MN, Youn G, Jones B, et al. Are vancomycin troughs adequate for optimal dosing? Antimicrob Agents Chemother. 2014;58:309–16.
Le J, Ngu B, Bradley JS, et al. Vancomycin monitoring in children using bayesian estimation. Ther Drug Monit. 2014;36:510–8.
Hurst AK, Yoshinaga MA, Mitani GH, Foo KA, Jelliffe RW, Harrison EC. Application of a Bayesian method to monitor and adjust vancomycin dosage regimens. Antimicrob Agents Chemother. 1990;34:1165–71.
Alsultan A, Abouelkheir M, Alqahtani S, et al. Optimizing vancomycin monitoring in pediatric patients. Pediatr Infect Dis J. 2018;37:880–5.
Stockmann C, Olson J, Rashid J, et al. An evaluation of vancomycin area under the curve estimation methods for children treated for acute pulmonary exacerbations of cystic fibrosis due to methicillin-resistant Staphylococcus aureus. J Clin Pharmacol. 2019;59:198–205.
Acknowledgments
The authors acknowledge financial support from the Researchers Supporting Project number (RSP-2019/39), King Saud University, Riyadh, Saudi Arabia.
Author information
Authors and Affiliations
Contributions
AbdullahA wrote part of the manuscript and did the pharmacokinetic analysis; MA designed the study and reviewed the manuscript; AhmadA did part of the pharmacokinetic analysis and reviewed the manuscript; EA and AhmedA collected the data and wrote part of the manuscript; SA designed the study and reviewed the manuscript. AbdullahA will act as guarantor for this paper.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Ethics Approval
The study was approved by the local Institutional Research Ethics Board at King Saud University Medical City.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Alsultan, A., Abouelkheir, M., Albassam, A. et al. AUC- vs. Trough-Guided Monitoring of Vancomycin in Infants. Indian J Pediatr 87, 359–364 (2020). https://doi.org/10.1007/s12098-019-03162-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-019-03162-5