
Abstract
Objective
To study the clinical profile of the Indian children admitted with DKA.
Methods
This descriptive retrospective study was conducted in pediatric ICU of tertiary level care hospital at Delhi (between Jan 2008 and Jan 2010). The case records of 55 children admitted with DKA were reviewed and information with respect to the personal details, clinical features, laboratory parameters, management and outcome was recorded using a predesigned performa.The data was analyzed using SPSS version 16.
Results
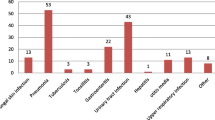
The mean age of patients at presentation was 7.4 ± 3.9 y; 27 boys and 28 girls were enrolled. Diabetes was newly diagnosed in 56.4% patients and 43.6% were known cases of diabetes. Polyuria and polydipsia (54.5%), persistent vomiting (52.7%), altered sensorium (50.9%), abdominal pains (47.3%) were common presenting symptoms. Most of the children had dehydration at admission, one fourth being severe. Hypernatremia, hypokalemia, cerebral edema and renal failure were observed in 20%, 14.5%, 14.5% and 7.2% , respectively. While 12.72% had fatal outcome, cerebral edema with or without renal failure and sepsis accounted for most of the deaths.
Conclusions
Boys and girls were equally affected. Newly diagnosed diabetics constituted more >50% of total DKA admissions. Nearly two third presented with severe DKA. Renal failure, cerebral edema and sepsis contributed to adverse outcome.
Similar content being viewed by others

References
Faich G, Fishbein H, Ellis E. The epidemiology of diabetic acidosis: a population-based study. Am J Epidemiol. 1983;117:551–8.
Dunger DB, Sperling MA, Acerini CL, et al. ESPE/LWPES consensus statement on diabetic ketoacidosis in children and adolescents. Arch Dis Child. 2004;89:188–94.
Burns MR, Bodansky HJ, Parslow RC. Pediatric intensive care admission for acute diabetes complications. Diabet Med. 2010;27:705–8.
Lone SW, Siddiqui EU, Muhammad F, Atta I, Ibrahim MN, Raza J. Frequency, clinical characteristic and outcome of diabetic ketoacidosis in children with type1 diabetes at a tertiary care hospital. J Pak Med Assoc. 2010;60:725–29.
Tubina-Rafi N, Habita C, Czernichow P. Critical study of diabetic ketoacidosis in children. Initial description and course during the first 24 hour of treatment. Arch Fr Pediatr. 1992;49:175–80.
Al-Mantrafi J, Vethamuthu J, Feber J. Acute renal failure in patient with diabetic ketoacidosis. Saudi J Kidney Dis Transpl. 2009;20:831–4.
Jayashree M, Singhi S. Diabetic ketoacidosis: predictors of outcome in a pediatric intensive care unit of a developing country. Pediatr Crit Care Med. 2004;5:427–33.
Wolfsdorf J, Glaser N, Sperling MA. Diabetic ketoacidosis in infants, children and adolescents:A consensus statement from American Diabetes Association. Diabetes Care. 2006;29:1150–9.
Glaser N. Pediatric diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Clin N Am. 2005;52:1611–35.
Contributions
S K: conceptualized the study, drafted and finalized the manuscript; AB:collected the patient data ; VK: reviewed the manuscript.
Conflict of Interest
None
Role of Funding Source
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kanwal, S.K., Bando, A. & Kumar, V. Clinical Profile of Diabetic Ketoacidosis in Indian Children. Indian J Pediatr 79, 901–904 (2012). https://doi.org/10.1007/s12098-011-0634-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-011-0634-3