
Abstract
Introduction
In patients with peritoneal carcinomatosis (PC), the incidence of respiratory complications following cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) is not well established. We aimed to describe the center-specific incidence and patient characteristics associated with respiratory complications following CRS and HIPEC in patients receiving treatment for PC.
Materials and methods
We used the University Hospital of Arrixaca study database to identify patients who underwent CRS and HIPEC for PC. Patients who experienced a post-operative respiratory complication were categorized according to the National Cancer Institute-Common Terminology Criteria for Adverse Events. Multivariable regression methods were used to identify independent risk factors for developing a respiratory complication following CRS and HIPEC.
Results
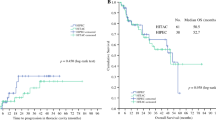
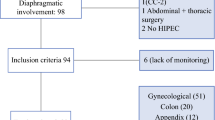
Between 2008 and 2017, we identified 247 patients who underwent CRS and HIPEC for PC. A total of eight patients (3.2%) were categorized as having a post-operative respiratory complication. A diaphragmatic peritonectomy and a PC index of > 14 were identified as independent risk factors for developing a respiratory complication. Radiographic evidence of a pleural effusion was identified in 72 patients who had CRS of the diaphragmatic peritoneum; however, only 6 (8.3%) of these patients required pleural drainage.
Conclusions
Only 3.2% of patients developed a symptomatic respiratory complication following CRS and HIPEC. A pleural effusion was identified in almost all patients requiring a diaphragmatic peritonectomy as part of their CRS; however, less than one in ten of these patients required pleural drainage. Prophylactic insertion of a pleural drainage tube is, therefore, not indicated following CRS and HIPEC.

Similar content being viewed by others

Abbreviations
- ASA:
-
American Society Anaesthesiologists
- CRS:
-
Cytoreductive surgery
- ECOG:
-
Eastern Cooperative Oncology score
- HIPEC:
-
Hyperthermic intraperitoneal chemotherapy
- INR:
-
International normalized ratio
- ITU:
-
Intensive care unit
- NCI-CTCAE:
-
National Cancer Institute-Common Terminology Criteria for Adverse Events
- OR:
-
Odds ratio
- PC:
-
Peritoneal carcinomatosis
- PCI:
-
Peritoneal carcinomatosis index
- SD:
-
Standard deviation
References
Hoskins WJ. Epithelial ovarian carcinoma: principles of primary surgery. Gynecol Oncol. 1994;55:S91–6. https://doi.org/10.1006/gyno.1994.1346.
Muñoz-Casares FC, Rufián S, Rubio MJ, Díaz CJ, Díaz R, Casado A, et al. The role of hyperthermic intraoperative intraperitoneal chemotherapy (HIPEC) in the treatment of peritoneal carcinomatosis in recurrent ovarian cancer. Clin Transl Oncol. 2009;11:753–9.
Shih KK, Chi DS. Maximal cytoreductive effort in epithelial ovarian cancer surgery. J Gynecol Oncol. 2010;21:75–80. https://doi.org/10.3802/jgo.2010.21.2.75.
Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, et al. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol Oncol. 2006;103:559–64. https://doi.org/10.1016/j.ygyno.2006.03.051.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. https://doi.org/10.3322/caac.21166.
Benedetti Panici P, Di Donato V, Fischetti M, Casorelli A, Perniola G, Musella A, et al. Predictors of postoperative morbidity after cytoreduction for advanced ovarian cancer: analysis and management of complications in upper abdominal surgery. Gynecol Oncol. 2015;137:406–11. https://doi.org/10.1016/j.ygyno.2015.03.043.
Eisenhauer EL, D’Angelica MI, Abu-Rustum NR, Sonoda Y, Jarnagin WR, Barakat RR, et al. Incidence and management of pleural effusions after diaphragm peritonectomy or resection for advanced mullerian cancer. Gynecol Oncol. 2006;103:871–7. https://doi.org/10.1016/j.ygyno.2006.05.023.
U.S. Department of Health and Human Services. National Institutes of Health. National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. Published: May 28, 2009 (v4.03: June 14, 2010). n.d.
Péus D, Newcomb N, Hofer S. Appraisal of the Karnofsky performance status and proposal of a simple algorithmic system for its evaluation. BMC Med Inform Decis Mak. 2013;13:72. https://doi.org/10.1186/1472-6947-13-72.
Gilly FN, Cotte E, Brigand C, Monneuse O, Beaujard AC, Freyer G, et al. Quantitative prognostic indices in peritoneal carcinomatosis. Eur J Surg Oncol. 2006;32:597–601. https://doi.org/10.1016/j.ejso.2006.03.002.
Sugarbaker PH. Management of peritoneal-surface malignancy: the surgeon’s role. Langenbeck’s Arch Surg. 1999;384:576–87.
Cliby W, Dowdy S, Feitoza SS, Gostout BS, Podratz KC. Diaphragm resection for ovarian cancer: technique and short-term complications. Gynecol Oncol. 2004;94:655–60. https://doi.org/10.1016/j.ygyno.2004.04.032.
Dowdy SC, Loewen RT, Aletti G, Feitoza SS, Cliby W. Assessment of outcomes and morbidity following diaphragmatic peritonectomy for women with ovarian carcinoma. Gynecol Oncol. 2008;109:303–7. https://doi.org/10.1016/j.ygyno.2008.02.012.
Chéreau E, Rouzier R, Gouy S, Ferron G, Narducci F, Bergzoll C, et al. Morbidity of diaphragmatic surgery for advanced ovarian cancer: retrospective study of 148 cases. Eur J Surg Oncol. 2011;37:175–80. https://doi.org/10.1016/j.ejso.2010.10.004.
Montz FJ, Schlaerth JB, Berek JS. Resection of diaphragmatic peritoneum and muscle: role in cytoreductive surgery for ovarian cancer. Gynecol Oncol. 1989;35:338–40. https://doi.org/10.1016/0090-8258(89)90074-7.
Chéreau E, Ballester M, Selle F, Cortez A, Pomel C, Darai E, et al. Pulmonary morbidity of diaphragmatic surgery for stage III/IV ovarian cancer. BJOG An Int J Obstet Gynaecol. 2009;116:1062–8. https://doi.org/10.1111/j.1471-0528.2009.02214.x.
Aletti GD, Dowdy SC, Gostout BS, Jones MB, Stanhope CR, Wilson TO, et al. Aggressive surgical effort and improved survival in advanced-stage ovarian cancer. Obstet Gynecol. 2006;107:77–85. https://doi.org/10.1097/01.AOG.0000192407.04428.bb.
Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002;20:1248–59. https://doi.org/10.1200/JCO.2002.20.5.1248.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors of the research article entitled “Identifying the incidence of respiratory complications following diaphragmatic cytoreduction and hyperthermic intraoperative intraperitoneal chemotherapy” declare that there are no potential conflicts of interest.
Ethical approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Cascales Campos, P., Martinez Insfran, L.A., Wallace, D. et al. Identifying the incidence of respiratory complications following diaphragmatic cytoreduction and hyperthermic intraoperative intraperitoneal chemotherapy. Clin Transl Oncol 22, 852–859 (2020). https://doi.org/10.1007/s12094-019-02195-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-019-02195-8