
Abstract
Purpose
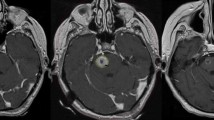
The incidence of brainstem metastasis (BSM) accounts for 1–3% of brain metastases (BM). They are often associated with multiple BM and produce significant neurological symptoms. We retrospectively analyse the results of treatment with stereotactic radiosurgery (SRS).
Methods and material
We included the medical records of 28 patients aged 52.86±11.29 years; 17 (60.7%) were women. The most frequent primary tumours were breast (n=11), lung (n=9) and melanoma (n=4). A total of 30 BSM were treated with radiosurgery (SRS) with a linear accelerator (Linac Scalpel, University of Florida). The 3D planning was with image fusion.
Results
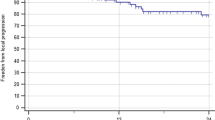
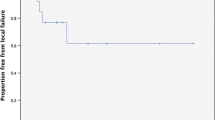
The mean time from the diagnosis of the primary tumour to the BM was 3±3.35 years; 5 cases were diagnosed simultaneously. Twenty-seven patients (96.4%) received whole brain radiotherapy, 19 before SRS and 8 after. The most usual dose was 30 Gy. Three patients underwent another SRS for other BM. The medium volume of BSM was 1.86±2.31 cc. The mean prescribed dose was 1114.33±315.6 cGy. The tumour volume did not change significantly with SRS but there was neurological improvement in 13 patients (41.9%). Twenty-four patients (85.7%) died, 22 (78.5%) due to the primary tumour: 12 cases (42.8%) due to progression of BM, 1 case due to progression of BSM and 10 due to local tumour progression or extra-cerebral metastases. Mean survival from diagnosis of BM was 22.8±32.4 months and from SRS of BSM, 16.8±31.56 months (1 month to 13.54 years).
Conclusion
The combined treatment of SRS and whole brain radiotherapy treatment is effective in the control of BSM (only one patient died due to progression of BSM), improving the neurological symptoms in 41.9% of patients; therefore an early diagnosis and treatment is important. Many patients die due to causes other than the BSM.
Similar content being viewed by others
References
Tsao MN, Lloyd NS, Wong RKS et al (2005) Radiotherapeutic management of brain metastases: a systematic review and meta-analysis. Cancer Treat Rev 31:256–273
Gaspar LE, Scott C, Murray K, Curran W (2000) Validation of the recursive partitioning analysis (RPA) classification for brain metastases. Int J Radiat Oncol Biol Phys 47:1001–1006
Bradley KA, Metha MP (2004) Management of brain metastases. Semin Oncol 31:693–701
Andrews DW, Scott CB, Sperduto PW et al (2004) Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to tree brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet 363:1665–1672
Aoyama H, Shirato H, Tago M et al (2006) Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases. A randomized controlled trial. JAMA 295:2483–2491
Metha MP, Tsa MN, Whelan TJ et al (2005) The American Society Therapeutic Radiology and Oncology (ASTRO) evidence-based review of the role of radiosurgery for brain metastases. Int J Radiat Oncol Biol Phys 63:37–46
Kondziolka D, Pate A, Lunsford LD et al (1999) Stereotactic radiosurgery plus whole brain radiotherapy versus radiotherapy alone for patients with multiple brain metastases. Int J Radiat Oncol Biol Phys 45:427–434
Bhatnagar AJ, Flickinger JC, Kondziolka D, Lunnsford D (2006) Stereotactic radiosurgery for four or more intracranial metastases. Int J Radiat Oncol Biol Phys 64:898–903
Hussain A, Brown PD, Stafford SL, Pollock BE (2007) Stereotactic radiosurgery for brainstem metastases: survival, tumor control, and patient outcomes. Int J Radiat Oncol Biol Phys 67:521–524
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Samblás, J.M., Sallabanda, K., Bustos, J.C. et al. Radiosurgery and whole brain therapy in the treatment of brainstem metastases. Clin Transl Oncol 11, 677–680 (2009). https://doi.org/10.1007/s12094-009-0423-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-009-0423-x