
Abstract
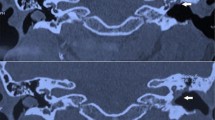
This study has aimed to determine the anatomical site of labyrinthine fistula in patients of chronic suppurative otitis media at our centre. Labyrinthine fistulae (LF) are caused by abnormal communications between the inner ear and surrounding structures resulting in perilymph leakage and hearing loss. Labyrinthine fistula represents as erosive loss of the enchondral bone overlying the semicircular canals without loss of perilymph. The manifestations of fistula like vertigo, hearing loss vary in severity and complexity, commonly ranging from very mild to incapacitating. Cholesteatoma induced fistula most commonly involves lateral semicircular canal probably because of its close proximity to the middle ear, but can involve other semicircular canals and rarely cochlea. This is a retrospective analysis of 36 patients of chronic suppurative otitis media with history of vertigo undergoing tympanomastoid surgery in whom there was an evidence of labyrinthine fistula on HRCT scan of temporal bone. The incidence of patients with labyrinthine fistula presenting with vertigo, nystagmus, sensorineural hearing loss, history of vertigo were analysed. The anatomical location of the fistula was supported by Radiological evidence. Patients underwent either canal wall down mastoidectomy or cortical mastoidectomy. The anatomical site and length of the labyrinthine fistula were analysed. Amongst the 36 patients of chronic suppurative otitis media with labyrinthine fistula 22 (61.1%) patients had atticoantral disease, 4 (11.1%) patients had chronic otitis media with extensive granulation, 2 (5.5%) patients had Tubotympanic disease with polyps, 4 (11.1%) patients had Tuberculous otitis media, 1 (2.77%) patient had Tubotympanic disease with extensive tympanosclerosis eroding the dome of lateral semicircular canal, 1 (2.77%) patient had extensive cholesteatoma with cerebellar abscess, 1 (2.77%) patient had fistula in the promontory following trauma, 1 (2.77%) patient had extensive tympanosclerosis with erosion of promontory. It was noticed that, in 14 (38.88%) patients the fistula was at the centre, in 17 (47.22%) patients the fistula is towards the ampullary end of horizontal semicircular canal and in 5 (13.88%) patients the fistula was towards the non ampullary end of lateral semicircular canal. The maximum length of fistula noticed was 6 mm and the minimum length of the fistula noticed was 2 mm. Labyrinthine fistula are most commonly noticed in the ampullary end of the lateral semicircular canal. The average length of the fistula was found to be 4 mm. Careful elevation of the cholesteatoma matrix over the endosteal membrane and immediate placement of temporal fascia over the exposed fistula is important to avoid injury to the inner ear. Maximum number of fistula were seen in the atticoantral type of Chronic suppurative otitis media. Prior knowledge of anatomical location of the fistulous tract in HRCT temporal bone is important to address the fistula.
Similar content being viewed by others


References
Minor LB (2003) Labyrinthine fistulae: pathobiology and management. Curr Opin Otolaryngol Head Neck Surg 11:340–346 (14502064)
Moon IS, Knon MO, Park CY, Hong SJ, Shim DB, Kim J et al (2012) Surgical management of labyrinthine fistula in chronic otitis media with cholesteatoma. Auris Nasus Larynx 39:261–264
Palva T, Ramsay H (1989) Treatment of labyrinthine fistula. Arch Otolaryngol Head Neck Surg 115:804–806
Copeland BJ, Buchman CA (2003) Management of labyrinthine fistulae in chronic ear surgery. Am J Otolaryngol 24(1):51–60
Fuse T, Tada Y, Aoyagi M, Sugai Y (1996) CT detection of facial canal dehiscence and semicircular canal fistula: comparison with surgical findings. J Comput Assist Tomogr 20(2):221–224
Cho CH, Yang HC, Aum JH, Kim YW, Hyoung Lee J (2014) Preservation of post operative bone conduction hearing after labyrinthine fistula repair in chronic otitis media with cholesteatoma: a review of 23 cases. Int Adv Otol 10(1):39–43
Stephenson MF, Saliba I (2011) Prognostic indicators of hearing after complete resection of cholesteatoma causing a labyrinthine fistula. Eur Arch Otorhinolaryngol 268(12):1705–1711
Gocea A, Martinez-vidal B, Panuschka C, Epprecht P, Caballero M, Bernal-sprekelsen M (2012) Preserving bone conduction in patients with labyrinthine fistula. Eur Arch Otorhinolaryngol 269(4):1085–1090
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Study was conducted after obtaining institutional ethical clearance. No conflicts of interest.
Ethical Approval
Institutional ethical committee clearance was obtained for this study.
Research Involving Human Participants and/or Animals
No.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Prasad, K.C., Vyshnavi, V., Abhilasha, K. et al. Labyrinthine Fistula-Our Experience at a Tertiary Hospital. Indian J Otolaryngol Head Neck Surg 74 (Suppl 1), 88–92 (2022). https://doi.org/10.1007/s12070-020-01857-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-020-01857-2