
Abstract
Recent changes in the pension system may contribute to larger social inequalities and more involuntary late retirement transitions due to financial need. Lower educated workers may have less control over their retirement and may need to stay in the labour market despite poor health. How different aspects of the retirement transitions are related to post-retirement health is unclear. This study investigates health differences across educational levels among 1280 retirees participating in the ‘Health, Ageing and Retirement Transitions in Sweden’ (HEARTS) study. Retirement age and involuntary reasons for retirement were considered as potential mediator and moderators of the social gradient in health outcomes. Results from a path analysis suggest that lower educated retirees are more likely to stop working for physical reasons, which is related to poor post-retirement health. Hence, involuntary retirement mediates the educational effect on health. Linear regressions highlighted the moderating effect of retirement age: lower educated retirees had worse health than higher educated retirees when their transitions were late. Hence, the double disadvantage of lower educated individuals becomes apparent. This study contributes to explaining possible mechanisms of rising health inequalities by focusing on aspects of retirement.
Similar content being viewed by others


Introduction
Adjusting to population ageing, the institutional context of retirement in Sweden has changed markedly throughout the last decades (Hamblin 2013; König and Lindquist 2016). Research suggests that the retirement timing has become more involuntary for certain social groups (Hofäcker et al. 2016) as an effect of the privatization and marketization of the pension system (Ebbinghaus 2015). Those with lower lifetime earnings and often those with lower education are forced to work longer to accumulate higher pension benefits in the current, reformed pension system. In addition, changes limiting the eligibility of disability pensions provide lower opportunities to exit the labour market earlier, despite strenuous working conditions which may pose a threat to physical and mental health. Hence, it is argued that certain work force segments, in more recent cohorts, have less choice and control over their retirement transition.
Some scholars argue that “control over one’s own life and the healthy lifestyle that goes with that control account for most of the association between education and health” (Mirowsky and Ross 2003, p. 49). The advantages of higher education tend to accumulate over the life course which implies that health differences across educational levels tend to become more pronounced in older ages. Previous studies have tried to disentangle the effects of cohort and age group differences and often report rising differences across educational levels, at least with regard to health in later born cohorts (Hu et al. 2016), which has been described as the “rising importance hypothesis” (Lynch 2003; Mirowsky and Ross 2008). There are also indications for the “cumulative advantage hypothesis”, proposing that differences in health and physical functioning related to education tend to increase with age (Leopold 2016; Leopold and Engelhartdt 2012; Lynch 2003; Mirowsky and Ross 2008; Schöllgen et al. 2010). Comparisons of the effects of educational background for health outcomes in older ages are therefore important.
In order to understand the mechanisms of the rising importance hypothesis, we also need to consider the effects of changes in the retirement system. It has been suggested that pension policies for later retirement ages may exacerbate health inequalities (Marshall and Nazroo 2016). In a recent call for future research on the relationship between socio-economic status and health, Corna (2013, p. 153) suggests that “in the context of the life course, too little attention is devoted to understanding how these socioeconomic inequalities are sustained, exacerbated or attenuated over time. This oversight leaves the institutional and structural factors that shape the experiences that are consequential for SEP [socio-economic position], and their subsequent relationship with health, largely unaddressed”. This notion is in line with the review on retirement timing which emphasizes the need for more research on social inequalities and retirement timing (Fisher et al. 2016).
Therefore, the present study aims to investigate the socioeconomic gradient in post-retirement health outcomes taking retirement age and reasons for retirement into account.
Mechanisms Behind the Accumulating Effects of Education on Health
Socioeconomic conditions are accompanied with health inequalities, which also tend to accumulate over the life span. The relationship between some measures of socioeconomic status (i.e. income and occupation) and health are easy to explain. Higher income is related to the financial ability to buy medical care and to attend health promoting activities. Certain occupations are related to strenuous working conditions which can lead to worse health. When it comes to education, a strong relationship with health and accumulating effects over the life course can be found (Batty et al. 2007; Beckett 2000; Leopold 2016; Leopold and Engelhartdt 201212; Schöllgen et al. 2010), but it is less obvious how the educational background affects health in late adulthood and aging. Mirowsky and Ross (2003) argue that education is related to higher control over one’s life which is related to better health. Control can be manifested both financially and behaviourally.
Education tends to increase the sense of control via knowledge or self-efficacy, which has an influence on risk and problem-solving behaviour (Bandura 1997; Pampel and Rogers 2004). Higher perceived control reduces distress caused by the feeling of helplessness (Marmot et al. 1998), increases the effort to avoid risks and is related to a higher awareness for health related behaviour such as exercise, diets, drinking and smoking. These behavioural or lifestyle aspects may also be related to biological accumulations (Mirowsky and Ross 2003).
The sense of control and physiological wellbeing is challenged in later life (Rodin 1986). Life events like widowhood, diseases, and forced retirement might decrease a person’s sense of control. At the same time, physical functioning tends to decrease which mutually reinforces decline in the sense of personal control.
Sense of Control over Retirement and Health Outcomes
Overall, perceived control is found to be related strongly to retirement adjustment (van Solinge and Henkens 2005) and can be seen as crucial for successful aging (Rowe and Kahn 1997). Quine et al. (2007) related low control and choice over the retirement transition to worse health and wellbeing over a 3 year period. They found an association between low control and low job status, which is typically observed among those with lower education.
In the retirement transition, a focus on sense of control becomes especially relevant when it comes to the factual circumstances of voluntary or involuntary retirement. Previous research show that involuntary retirement is likely to be related to negative health outcomes, decline in life satisfaction and self-efficacy (Dingemans and Henkens 2015), an increased risk of depression (Hyde et al. 2015), lower happiness (Calvo et al. 2009) and to a decrease in self-rated health (Dave et al. 2008; van Solinge 2007). Rationally, the decision to retire is made by economic considerations (Laitner and Sonnega 2013). Involuntary retirement could therefore also be associated with insufficient financial savings that prevent a healthy life style, which in turn, might produce worse health.
Retirement or exits from the workforce represent a critical life event, and as Rodin (1986) mentioned, forced retirement can be related to a lower sense of control. Recently, it is argued that social inequalities in retirement might be rising (Ebbinghaus 2015) due to inequity issues of increasing retirement ages (Harper et al. 2011). Lower educated persons are likely to exert less control over their retirement transition since they need to work longer to accumulate a sufficient pension income. Hence, late retirement is suggested to be less voluntary among lower educated workers (Madero-Cabib and Kaeser 2015).
Taking the example of Sweden, the necessity to work longer is even institutionalized by the pension system. While the statutory pension age was flexibilized and allowed for early exits often combined with occupational pensions, the guaranteed pension (Swedish: garantipension) can still only be withdrawn at the age of 65 years. Groups with lower socio-economic status will not have a high occupational pension to leave earlier and are more likely to rely on guaranteed pension. Additionally, disability pensions were broadly used especially by lower educated workers as early retirement pathway before the far-reaching reforms in the late 1990s (Sjögren Lindquist 2013), when the eligibility rules became more restricted. This option to early retirement was closed for many lower educated individuals (König and Lindquist 2016). Since 1997, it is impossible to leave on disability pensions for labour market reasons, only for health reasons. A report by Tåhlin (2011) finds that those with low job quality were much more likely to exit the labour market in earlier cohorts compared to today. He relates this finding to changes in disability pensions in Sweden. Halleröd et al. (2012) investigated earlier cohorts and found a strong relationship between early exit routes (disability pensions, sickness benefits, unemployment benefits) and decreasing health after retirement. They conclude that post-retirement health and well-being is related mainly to pre-retirement conditions, not to the transition itself. However, they acknowledge that recent developments in the eligibility restrictions of disability pensions might present a different context and should be investigated in future research. Hence, nowadays it might be more important to focus on the variance among those who did not receive disability or sickness benefits to facilitate early labour market exits.
The Relationship Between Retirement, Socio-Economics, and Health
Changes in the pension system may have an effect on inequalities in health after retirement depending on education. A study by Coe et al. (2012) on cognitive change following retirement found that the transition to retirement had a beneficial effect only among blue-collar workers. Eibich (2015) finds that only lower educated individuals show improved physical health after retirement and relates this finding to the relief from physical work strain that often characterizes lower qualified jobs. Beyond physical work strain, Westerlund et al. (2009) show that retirement leads to an improvement of health for those in poor working conditions – including both high physical/psychological demands and low job satisfaction – who reported health complaints before retirement. This improvement was not found for those with better job quality and higher occupational classes. These results were confirmed by Matthews (2014) who also found that retirement was related to an improvement in self-rated health and cognitive function among those in low quality jobs. Matthews even finds a decrease in health and functioning for those in high quality jobs following retirement. Similar results were found by Marshall and Nazroo (2016).
Overall, it may be concluded that retirement from strenuous, low quality jobs seems to lead to an improvement of physical health while the opposite might be true for high quality jobs and those with high job satisfaction. Thus, we may expect that retirement is related to improved physical health in lower educated and blue collar workers, but not in more highly educated white collar workers.
A framework by Calvo et al. (2013) differentiates contrasting outcomes of subjective health by the timing of retirement in order to account for competing hypotheses. However, little is known about this relationship, opposing results can be found and there is no explicit differentiation by subgroups. Eibich (2015) concludes that the positive effect of retirement on mental health is driven by those retiring after the age of 65 years. The effect is not significant for those retiring earlier at age 60 years. Rohwedder and Willis (2010) related early retirement to worse cognitive functioning and explained this finding by the involvement in a stimulating work environment. Wu et al. (2016) investigated mortality and found that later retirement was associated with lower risks of mortality, independent of socio-demographic or health determinants. They also found that unhealthy retirees had lower mortality risks when they retired later. These studies indicate a beneficial effect of late retirement.
Other studies, however, suggest positive effects of early retirement on health since job related stress decreases and opportunities for exercises increase (Jokela et al. 2010; Westerlund et al. 2009). Jokela et al. (2010) find that voluntary early retirement is related to better mental health and physical functioning. Their results indicated that early retirement has a causal effect on better health since reverse causality would suggest that those with poor health retire early and therefore have worse health after retirement. A longitudinal study suggests that those who retire early had a steeper increase of the prevalence for illness before retirement compared to after retirement. The opposite was true for those who retired late (Marshall and Nazroo 2016). Some studies suggest that retirement timing is not related to health after retirement (Butterworth et al. 2006; van Solinge 2007), but the contradictory findings on retirement timing might be related to a general and too undifferentiated view on retirement in which social differences are not taken into account. The present study aims to close this gap by investigating retirement transitions in various educational groups. As research on socio-economic differences with regard to retirement and health suggests, retirement from low quality jobs should be beneficial. Hence, early retirement should be related to better health for lower educated (in low quality jobs) compared to later retirement. Furthermore, this should be even more pronounced if early retirement was voluntary.
In sum, the reviewed research on the relationship between retirement and the associated dimensions of health, personal control, and education suggest that a) lower educated retirees experience worse health compared to higher educated retirees, and b) lower control over the retirement transition is related to worse health, and c) lower educated are more likely to experience lower control over the retirement transition.
The consistent results from previous studies on the role of exit work characteristics made us not to focus on individual retirement transitions, rather on differences between groups of individuals with lower and higher education. In addition, we include timing and voluntariness of retirement to provide a more detailed understanding of the effects of retirement transitions.
Given the context of our study and previous results, we propose the following hypotheses:
Hypothesis 1: We expect perceived control over retirement and the voluntariness of transitions to mediate the negative relationship between lower education and health.
Hypothesis 2a: We expect that retirement age moderates the negative relationship between low education and health.
Hypothesis 2b: We expect that retirement age moderates the negative relationship between low education and health, especially when retirement transitions are involuntary.
Method
To investigate health differences across educational levels for the age group around 60 years, we used data drawn from the “Health, Ageing and Retirement Transitions in Sweden” (HEARTS) study (Lindwall et al. 2017), conducted at the University of Gothenburg. A nationally representative sample of 14,990 individuals was recruited through the register Statens personadressregister (SPAR). In total, 5913 individuals in the age range 60–66 years answered a web-based or paper-pencil version of a comprehensive battery designed to cover relevant aspects of the retirement transition.
Sample
The HEARTS sample consists of working and retired people. We limit the sample to retirees with reported retirement age, which were 1491 in total. Thereof, 38 had missing information on gender, education or self-reported health. Furthermore we excluded 80 individuals with a retirement age below 60. Last, 93 individuals did not response the questions for the voluntariness of retirement, i.e. the reasons for retirement which is partly due to a differentiation between those who receive pensions but continued working. Our final sample consists of 1280 individuals (Table 1).
Analysis
For investigating whether the effect from education on health is mediated by the voluntariness of retirement transitions, a structural equation model was conducted using PROCESS for SPSS (Hayes 2012). Indirect effects were examined using a bootstrapping resampling approach, using 1000 bootstrap samples.
To test the complex relationships between education, retirement age, and voluntariness of retirement transitions, ordinary least square (OLS) regressions on self-reported health were conducted including three-way interactions (retirement age, three measures of control over transition and education) and a quadratic term for retirement age to test a u-shaped relationship.
Measures
Health is assessed with a self-reported measure on subjective health. The item “how do you evaluate your overall health condition?” could be rated on a 6-point scale, reaching from very bad to very good. On average, the sample is in rather good health with a mean value of 4.75.
Education is measured as highest educational level based on 7 groups. A dummy variable for low education was coded 1 if the highest educational group was less than 9 years of education or basic education (Swedish: grundskola). An educational level higher than basic education was coded 0. Around 18% had a lower education in our sample.
Voluntariness of retirement transitions is captured by three variables: the control over retirement transitions, health related reasons for retirement and the feeling that work became too physically demanding as mentioned reason for retiring. All measures consisted of a 5-point scale. We argue that these three measures reflect distinct aspects of the voluntariness of retirement where the individual choice of the timing of transitions was restricted. Each measure was used separately in the analysis.
Retirement age is assessed via the date of retirement and date of birth. Lower retirement ages than 60 years are dropped (n = 80) due to the high selectivity of this group, i.e. their high likelihood to exit the labour force due to high wealth or disability.
Age in 2015 is included in years and ranged between 60 and 66 years. Gender is coded 1 if the respondent was female and it is coded 0 if the respondent was male.
Results
In a first step, we test the mediation of the effect of education on post-retirement health by different aspects of the retirement transition. Hence we test if lower education is related to worse health because it is related to certain aspects of retirement which are in turn related to poor health. Results show that higher education is significantly related to better health and less physical reasons for retirement. Education was not related to retirement age, health reasons for retirement and control over retirement. Physical reasons, health reasons and low control were related to poor post-retirement health. Physical reasons showed the only significant indirect effect between education and health (b = .021, 95% CI [0.014, 0.031]) and mediated the effect. In other words, low education is related to worse post-retirement health because it leads to involuntary retirement transitions and not being physically able to continue work. This provides partial evidence for hypothesis 1. The total indirect effect was significant (b = .030, 95% CI [0.015, 0.045]). However, a direct effect of education on health remains (b = .050, 95% CI [.025, 0.075]). It can be argued that the three measures of voluntariness can be seen as indicators for pre-retirement health. Hence, taking indirect effects into consideration, the effect from education on health cannot be completely explained. Worse post-retirement health among lower educated is not only due to a selection into different aspects of the retirement transition (Fig. 1).

Mediation model, direct effects
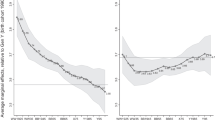
In the second step, we test the interaction effect of retirement age and education. We find some support for hypothesis 2a. A higher retirement age is related to worse health in lower educated individuals (Model 2 – linear measure of education: b = .015, p = 0.052; Model 3 – dummy variable for low education: b = −.141, p = 0.000). For visualization, Fig. 2 shows the marginal effects (95% CI) for education as a dummy variable on health at different retirement ages (Table 2).

Marginal effects on health: interaction between education and retirement age
The previous consistent finding that involuntary retirement is related to worse health outcomes was also confirmed by our results (Model 1). By our inclusion of an interaction term of physical reasons and education, we also find evidence that retirement for physical reasons is related to significantly worse health for lower educated retirees (Model 4: b = 13.27, p = 0.015).
Including a tree-way interaction of education, retirement age and physical reasons for retirement, our results show that late retirement is related to worse health for low educated retirees, especially when retirement transitions had physical reasons (Model 4: b = −.207, p = 0.017). This finding supports hypothesis 2b. For visualization, Fig. 3 shows the marginal effects (95% CI), using a dummy variable for physical reasons for retirement with the value 1 for highly involuntary retirement. In sum, among lower educated, health is suggested to be worse with later (involuntary) retirement transitions.

Marginal effects on health: interaction between education, retirement age and physical reasons for retirement
Linear regressions on health including interaction terms clarify the complex relationship between education and health outcomes. By allowing for a u-shaped relationship of retirement age, our analysis predicts a more accurate estimation of late and early retirement. Notably, we find that early and late retirement is associated with worse health. It becomes clear, however, that especially for lower educated individuals, higher retirement age is related to significantly worse health. This notion is even more apparent when transitions are involuntary. Since involuntary retirement may partly capture health related reasons for retirement and thereby pre-retirement health, it can be concluded that later transitions are particularly related to worse health among lower educated retirees when they had poor health during their last period at work.
Discussion and Conclusion
The present study was designed to analyse the social gradient in health outcomes, taking education, retirement age, and reasons for retirement into account. Participants were drawn from the ‘Health, Ageing and Retirement Transitions in Sweden’ (HEARTS) study.
The cross-sectional analyses conducted in our study prevent firm causal conclusions. However, reverse causality can be expected to provide opposite results and is therefore not very likely. Reverse causality would suggest that health produce a specific retirement timing, rather than being an outcome of retirement. In this case, those with ill-health can be expected to be selected into early retirement (Jokela et al. 2010; Madero-Cabib et al. 2016). The phenomenon of the healthy worker effect suggests that only healthy workers in fact are in the workforce and remain employed in older ages. Early retirement due to poor health should be related to worse health after retirement compared to late retirees. This is not the case for lower educated individuals. Higher retirement ages among lower educated individuals are related to worse health, which suggests that they might continue working despite poor health. Relating this to the pension context, it is quite likely that lower educated have less options to retire early due to insufficient pension income. This phenomenon may be described as the “unhealthy older worker effect” which needs to be addressed in more detail in future research. While this issue has been addressed in previous research (Marshall and Nazroo 2016), there are no studies investigating the effect of involuntary late retirement on health across different educational groups.
In the mediation model, we can be criticized for the fact that education and voluntariness of retirement are retrospective measures and not capturing the opportunities of the longitudinal design such as a direct measure of pre-retirement health. However, education refers to early life schooling, while voluntariness refers to the previous retirement transition of the sample, while health is reported after the transition. Acknowledging the limitations in using retrospective measures, causal conclusions are drawn in the discussion. Analysis of longitudinal data circumvents these difficulties but they are likely to be impaired by low sample sizes. Our analysis demands differentiation by education, retirement age and voluntariness of retirement which is only possible with large longitudinal datasets.
It is not possible to control for time in retirement since this is highly negatively correlated with retirement age due to the narrow and restricted age range of our sample (60 to 66 years old). Hence, the presented results could also be related to a retirement shock that may be more pronounced among lower educated retirees. While we acknowledge that this potential shock might exaggerate our findings, it is unlikely that it can account for the main findings. Previous longitudinal research rather suggests that retirement leads to an improvement for lower educated individuals, which furthermore suggests that a stronger retirement shock among lower educated is not very likely. Future research may address this issue by keeping time in retirement fixed and by using longitudinal data.
This study contributes to previous research in various ways. It highlights the importance of considering the effect of the actual retirement age, often neglected in previous studies. Halleröd et al. (2012) come to the conclusion that the retirement transition – measured by different pathways into retirement – does not play a role for post-retirement health. Our study sheds more light on the more recent developments in the Swedish pension system including the restrictions of early retirement and the flexibilization of pension age. Concluding from our results, retirement transitions may play a strong role for post-retirement health, although only for a certain group of retirees. Higher retirement ages are related strongly to worse health among lower educated individuals. This is even accelerated if transitions were involuntary. Hence, retirement timing and the element of voluntariness need to be considered when discussing the effect transitions from work to retirement on health. Our results further suggest that health inequalities across educational level may become more pronounced by involuntary late retirement. This contributes to research on the mechanisms of the accumulation of health differences over the life-course.
Our study sheds more light on the relationship between control, education and health. While it was previously suggested that lower education is related to lower control over retirement (Madero-Cabib and Kaeser 2015), this was partly confirmed in our Swedish sample. Even though the effect of control over retirement was not related to education, leaving for physical reasons can be seen as involuntary and without control. If a person would like to continue working but retires since they are unable to continue for physical reasons, they have less control over the transition. Hence, this type of involuntary reason for retirement was indeed found to be related to worse health and it mediated the effect of education on health.
Butterworth et al. (2006) and van Solinge (2007) do not find a relationship between retirement timing and health. Our study provides a more differentiated view. For the majority of individuals (i.e. those with higher education) retirement timing seems not to have any major impact on post-retirement health. However, in lower educated individuals we found a greater effect of retirement timing. The specific context of the Swedish pension system might generate these findings. While higher educated are more likely to have higher state pensions and additionally high occupational pensions, they have more control over their retirement timing. They may decide to leave earlier or stay longer, depending on their preference and ability. Lower educated might need to stay longer if their occupational pensions combined with their reduced state pensions are not sufficient for early retirement before age 65 years. Otherwise, they may need to work at least until age 65 if they rely on the guaranteed pension.
Our finding that educational differences in health seems to become significant only among those who retire late, may indicate that lower educated workers have to continue working despite poor health, which negatively affects further health after retirement. Previous research suggests that retirement should lead to a stronger improvement of health for lower educated workers compared to higher educated individuals. If this is the case, our results suggest that lower educated with poor health before retirement may not benefit from the positive effect of retirement if they delay their work exit. Educational differences are smaller and less significant when transitions were voluntary, i.e. not related to problems with physical work demands. Further longitudinal analyses are needed to clarify various transition patterns.
The theoretical contribution of our study is that it provides a better understanding of underlying mechanisms for the “rising importance hypothesis” and the “cumulative advantage hypothesis”, considering retirement transitions as critical life event. If involuntary late exits among lower educated workers is an outcome of recent changes in the pension system (Hofäcker et al. 2016) and related to greater health differences, it helps us to better explain the “rising importance hypothesis”. Our findings on a mediating effect of voluntariness in retirement transitions partly explain the effect from education on health and contribute to our understanding of the “cumulative advantage hypothesis”.
Finally, our study may have political implications. The double disadvantage of lower educated individuals in the current, reformed Swedish pension system becomes apparent: they are more likely to retire involuntarily which is related to worse health; and they have significantly worse health when they (have to) retire late. This may be important for concerns about equity issues centred around policies on increasing retirement ages (Harper et al. 2011).
References
Bandura, A. (1997). Self-efficacy: The exercise of control. Worth Publishers.
Batty, G. D., Deary, I. J., & Gottfredson, L. S. (2007). Premorbid (early life) IQ and later mortality risk: systematic review. Annals of Epidemiology, 17(4), 278–288. https://doi.org/10.1016/j.annepidem.2006.07.010.
Beckett, M. (2000). Converging health inequalities in later life--an artifact of mortality selection. Journal of Health and Social Behavior, 41(1), 106–119.
Butterworth, P., Gill, S. C., Rodgers, B., Anstey, K. J., Villamil, E., & Melzer, D. (2006). Retirement and mental health: analysis of the Australian national survey of mental health and well-being. Social Science & Medicine, 62(5), 1179–1191. https://doi.org/10.1016/j.socscimed.2005.07.013.
Calvo, E., Haverstick, K., & Sass, S. A. (2009). Gradual retirement, sense of control, and retirees’ happiness. Research on Aging, 31(1), 112–135. https://doi.org/10.1177/0164027508324704.
Calvo, E., Sarkisian, N., & Tamborini, C. R. (2013). Causal effects of retirement timing on subjective physical and emotional health. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 68(1), 73–84. https://doi.org/10.1093/geronb/gbs097.
Coe, N. B., von Gaudecker, H.-M., Lindeboom, M., & Maurer, J. (2012). The effect of retirement on cognitive functioning. Health Economics, 21(8), 913–927. https://doi.org/10.1002/hec.1771.
Corna, L. M. (2013). A life course perspective on socioeconomic inequalities in health: a critical review of conceptual frameworks. Advances in Life Course Research, 18(2), 150–159. https://doi.org/10.1016/j.alcr.2013.01.002.
Dave, D., Rashad, I., & Spasojevic, J. (2008). The effects of retirement on physical and mental health outcomes. Southern Economic Journal, 75(2), 497–523.
Dingemans, E., & Henkens, K. (2015). How do retirement dynamics influence mental well-being in later life? A 10-year panel study. Scandinavian Journal of Work, Environment & Health, 41(1), 16–23. https://doi.org/10.5271/sjweh.3464.
Ebbinghaus, B. (2015). The privatization and marketization of pensions in Europe: a double transformation facing the crisis. European Policy Analysis, 1(1). https://doi.org/10.18278/epa.1.1.5.
Eibich, P. (2015). Understanding the effect of retirement on health: mechanisms and heterogeneity. Journal of Health Economics, 43, 1–12. https://doi.org/10.1016/j.jhealeco.2015.05.001.
Fisher, G. G., Chaffee, D. S., & Sonnega, A. (2016). Retirement timing: a review and recommendations for future research. Work, Aging and Retirement, 2(2), 230–261. https://doi.org/10.1093/workar/waw001.
Halleröd, B., Örestig, J., & Stattin, M. (2012). Leaving the labour market: the impact of exit routes from employment to retirement on health and wellbeing in old age. European Journal of Ageing, 10(1), 25–35. https://doi.org/10.1007/s10433-012-0250-8.
Hamblin, K. (2013). Active ageing in the European Union: Policy convergence and divergence. UK: Basingstoke.
Harper, S., Howse, K., & Baxter, S. (2011). Living longer and prospering. Designing an Adequate, Sustainable and Equitable UK State Pension System. Prieiga per Internetą:< Ageing, Ox. Ac. Uk/System/Files/110110% 20Living% 20Longer% 20and% 20prospering, 20.
Hayes, A. F. (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling [White paper]. http://www.afhayes.com/public/process2012.pdf Accessed 03 11 2017.
Hofäcker, D., Hess, M., & König, S. (Eds.). (2016). Delaying retirement. London: Palgrave Macmillan UK.
Hu, Y., Lenthe, F. J. van, Borsboom, G. J., Looman, C. W. N., Bopp, M., Burström, B., … Mackenbach, J. P. (2016). Trends in socioeconomic inequalities in self-assessed health in 17 European countries between 1990 and 2010. Journal of Epidemiology and Community Health, 70(7), 644–652. https://doi.org/10.1136/jech-2015-206780.
Hyde, M., Hanson, L. M., Chungkham, H. S., Leineweber, C., & Westerlund, H. (2015). The impact of involuntary exit from employment in later life on the risk of major depression and being prescribed anti-depressant medication. Aging & Mental Health, 19(5), 381–389. https://doi.org/10.1080/13607863.2014.927821.
Jokela, M., Ferrie, J. E., Gimeno, D., Chandola, T., Shipley, M. J., Head, J., … Kivimäki, M. (2010). From midlife to early old age: Health trajectories associated with retirement. Epidemiology (Cambridge, Mass.), 21(3), 284–290. 10.1097/EDE.0b013e3181d61f53.
König, S., & Lindquist, G. S. (2016). Sweden: Steeply rising older workers’ employment rates in a late-exit country. In D. Hofäcker, M. Hess, & S. König (Eds.), Delaying retirement (pp. 315–335). UK: London. https://doi.org/10.1057/978-1-137-56697-3_14.
Laitner, John, and Amanda Sonnega. (2013). Economic theories of retirement. In the Oxford handbook of retirement edited by Wang, Mo. Oxford: Oxford University Press.
Leopold, L. (2016). Cumulative advantage in an egalitarian country? Socioeconomic health disparities over the life course in Sweden. Journal of Health and Social Behavior, 57(2), 257–273. https://doi.org/10.1177/0022146516645926.
Leopold, L., & Engelhartdt, H. (2012). Education and physical health trajectories in old age. Evidence from the survey of health, ageing and retirement in Europe (SHARE). International Journal of Public Health. https://doi.org/10.1007/s00038-012-0399-0.
Lindwall, M., Berg, A.-I., Bjälkebring, P., Buratti, S., Hansson, I., Hassing, L., Henning, G., Kivi, M., König, S., Thorvaldsson, V., & Johansson, B. (2017). Psychological health in the retirement transition: rationale and first findings in the HEalth, ageing and retirement transitions in Sweden (HEARTS) study. Frontiers in Psychology, 8. https://doi.org/10.3389/fpsyg.2017.01634.
Lynch, S. M. (2003). Cohort and life-course patterns in the relationship between education and health: a hierarchical approach. Demography, 40/2003(2), 309–331. https://doi.org/10.1353/dem.2003.0016.
Madero-Cabib, I., & Kaeser, L. (2015). How voluntary is the active ageing life? A life-course study on the determinants of extending careers. European Journal of Ageing, 13(1), 25–37. https://doi.org/10.1007/s10433-015-0355-y.
Madero-Cabib, I., Gauthier, J.-A., & Le Goff, J.-M. (2016). The influence of interlocked employment–family trajectories on retirement timing. Work, Aging and Retirement 2,(1), 38–53. https://doi.org/10.1093/workar/wav023.
Marmot, M. G., Fuhrer, R., Ettner, S. L., Marks, N. F., Bumpass, L. L., & Ryff, C. D. (1998). Contribution of psychosocial factors to socioeconomic differences in health. The Milbank Quarterly, 76(3), 403–448. https://doi.org/10.1111/1468-0009.00097.
Marshall, A., & Nazroo, J. (2016). Trajectories in the prevalence of self-reported illness around retirement. Journal of Population Ageing, 9(1–2), 11–48. https://doi.org/10.1007/s12062-015-9130-2.
Matthews, K. (2014). Is working beyond state pension age beneficial for health? Evidence from the English longitudinal study of ageing. Manchester: University of Manchester.
Mirowsky, J., & Ross, C. E. (2003). Education, social status, and health (Vol. 2003). Transaction Publishers.
Mirowsky, J., & Ross, C. E. (2008). Education and self-rated health cumulative advantage and its rising importance. Research on Aging, 30(1), 93–122. https://doi.org/10.1177/0164027507309649.
Pampel, F. C., & Rogers, R. G. (2004). Socioeconomic status, smoking, and health: a test of competing theories of cumulative advantage. Journal of Health and Social Behavior, 45(3), 306–321. https://doi.org/10.1177/002214650404500305.
Quine, S., Wells, Y., De Vaus, D., & Kendig, H. (2007). When choice in retirement decisions is missing: qualitative and quantitative findings of impact on well-being. Australasian Journal on Ageing, 26(4), 173–179. https://doi.org/10.1111/j.1741-6612.2007.00251.x.
Rodin, J. (1986). Aging and health: effects of the sense of control. Science, 233(4770), 1271–1276. https://doi.org/10.1126/science.3749877.
Rohwedder, S., & Willis, R. J. (2010). Mental retirement. The Journal of Economic Perspectives, 24(1), 119–138. https://doi.org/10.1257/089533010797456247.
Rowe, J. W., & Kahn, R. L. (1997). Successful aging. The Gerontologist, 37(4), 433–440. https://doi.org/10.1093/geront/37.4.433.
Schöllgen, I., Huxhold, O., & Tesch-Römer, C. (2010). Socioeconomic status and health in the second half of life: findings from the German ageing survey. European Journal of Ageing, 7(1), 17–28. https://doi.org/10.1007/s10433-010-0140-x.
Sjögren Lindquist, G. (2013). Flexibla arbetstider och utträde från arbetsmarknaden [Flexible working hours and exit from the labor market]. Statens Offentliga Utredningar 2011:05, Pensionsåldersutredningen.
Tåhlin, M. (2011). Arbetslivskarriärer bland kvinnor och män i Sverige 1974–2010 [Working life careers among women and men in Sweden 1974–2010]. Statens Offentliga Utredningar 2011:05, Pensionsåldersutredningen.
van Solinge, H. (2007). Health change in retirement a longitudinal study among older Workers in the Netherlands. Research on Aging, 29(3), 225–256. https://doi.org/10.1177/0164027506298223.
van Solinge, H., & Henkens, K. (2005). Couples’ adjustment to retirement: a multi-actor panel study. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 60(1), S11–S20. https://doi.org/10.1093/geronb/60.1.S11.
Westerlund, H., Kivimäki, M., Singh-Manoux, A., Melchior, M., Ferrie, J. E., Pentti, J., Jokela, M., Leineweber, C., Goldberg, M., Zins, M., & Vahtera, J. (2009). Self-rated health before and after retirement in France (GAZEL): a cohort study. The Lancet, 374(9705), 1889–1896. https://doi.org/10.1016/S0140-6736(09)61570-1.
Wu, C., Odden, M. C., Fisher, G. G., & Stawski, R. S. (2016). Association of retirement age with mortality: a population-based longitudinal study among older adults in the USA. Journal of Epidemiology and Community Health, 70(9), 917–923. https://doi.org/10.1136/jech-2015-207097.
Acknowledgements
This research has been funded by the Swedish Research Council for Health, Working Life and Welfare (FORTE), Dnr 2013-2291 and Dnr 2013-2300.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
König, S., Lindwall, M. & Johansson, B. Involuntary and Delayed Retirement as a Possible Health Risk for Lower Educated Retirees. Population Ageing 12, 475–489 (2019). https://doi.org/10.1007/s12062-018-9234-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12062-018-9234-6