
Abstract
Objectives
Heart transplantation has become an established procedure in India with increasing numbers being done annually. The majority of these patients are very sick with a history of multiple hospital admissions. The economic burden of such therapy is substantial and the costs are borne by the patients with very little insurance coverage. The objective of this study was to estimate the following:
-
1.
The average cost of a heart transplant procedure in a “real-world setting” in a private healthcare facility in India, with varying patient risk profiles.
-
2.
Identify the factors contributing to the wide variations in cost seen in practice.
-
3.
Finally, based on data thus collected, can some kind of estimation be made about the expected cost in a given patient before the operation is done?
Methods
The cost incurred by the hospital in doing 168 heart transplants during a 3-year period was analyzed. Costs were divided into direct and indirect costs. The direct costs consisted of medical consumables, laboratory investigations, radiology, costs involved in organ harvest and transport, and diet. Direct cost was 40 % of the total cost of the procedure and was used as a surrogate for total costing estimates.
Results
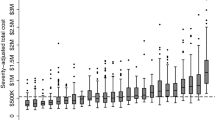
There was a wide variation in direct costs almost tenfold, ranging from INR 240,882 to 2403193 with a mean of 603755.The cost was affected by length of stay in the hospital, whether a patient survived or died and whether the patient died within 7 days of surgery or later. It was also affected by patient-specific factors like the INTERMACS status and preoperative creatinine levels. The average cost of the entire transplant procedure was INR 1459000.
Conclusion
There is a wide variation in the cost incurred by the hospital in doing transplants dictated to a large extent by patient risk profiles. A “One package fits all model” is unrealistic. The data pertains to the cost to the hospital and not the hospital bill and is therefore relevant to any health care facility, public or private. This study provides a framework for Governmental and private insurance agencies to fix the reimbursement rates.











Similar content being viewed by others


References
Chief Minister’s Comprehensive Health Insurance Scheme. [cited 2020 Jun 8]. Available from: https://www.cmchistn.com/
Wasserstein RL, Schirm AL, Lazar NA. Moving to a world beyond “ p < 0.05”. Am Stat. 2019;73:1–19 Available from: https://www.tandfonline.com/doi/full/10.1080/00031305.2019.1583913.
Amrhein V, Greenland S. Remove, rather than redefine, statistical significance. Nat Human Behav. 2018. https://doi.org/10.1038/s41562-017-0224-0.
Heart comes for free but transplant cost hits patients | Bengaluru News - Times of India. [cited 2020 Jun 8]. Available from: https://timesofindia.indiatimes.com/city/bengaluru/Heart-comes-for-free-but-transplant-cost-hits-patients/articleshow/51819396.cms
Emanuel EJ, Emanuel LL. The economics of dying -- the illusion of cost Savings at the end of life. New Eng J Med. 1994;330:540–4.
Home | Ayushman Bharat | National Health Authority | GoI. [cited 2020 Jun 8]. Available from: https://www.pmjay.gov.in/
Goldraich LA, Neyeloff JL, da Silva Etges APB, et al. Heart transplantation cost composition in Brazil: a patient-level microcosting analysis and comparison with international data. J Card Fail. 2018;24:860–3.
Fine MJ, Pratt HM, Obrosky DS, et al. Relation between length of hospital stay and costs of care for patients with community-acquired pneumonia. Am J Med. 2000;109:378–85.
Evans RW. The economics of heart transplantation. Circulation. 1987;75:63–76 Available from: https://www.ahajournals.org/doi/10.1161/01.CIR.75.1.63.
Cope JT, Kaza AK, Reade CC, et al. A cost comparison of heart transplantation versus alternative operations for cardiomyopathy. Ann Thorac Surg. 2001;72:1298–305.
Tan SS, Bakker J, Hoogendoorn ME, et al. Direct cost analysis of intensive care unit stay in four European countries: applying a standardized costing methodology. Value Health. 2012;15:81–6.
Edbrooke D, Hibbert C, Ridley S, Long T, Dickie H. The development of a method for comparative costing of individual intensive care units. Anaesthesia. 1999;54:110–20 Available from: http://doi.wiley.com/10.1046/j.1365-2044.1999.00650.x.
Krishnan KB, Rao KS, Tanguturu MK, et al. Commercial airlines as a viable, safe and cost effective way for transporting the donor hearts across the country: single center experience. J Heart Lung Transplant. 2019;38:S133–4.
Koster‐Brouwer ME, Klein Klouwenberg PM, Pasma W, Poll T, Bonten MJ, Cremer OL. Criticial care management of sepsis: a cost‐analysis from a health care perspective. Eur Soc Intensive Care Med. 2014;40:S1–S308.
Mercier G, Naro G. Costing hospital surgery services: the method matters. PLoS ONE. 2014;9:e97290 Available from: https://dx.plos.org/10.1371/journal.pone.0097290.
Chatterjee S, Laxminarayan R. Costs of surgical procedures in Indian hospitals. BMJ Open. 2013;3:e002844 Available from: http://bmjopen.bmj.com/lookup/doi/10.1136/bmjopen-2013-002844.
Acknowledgments
Our sincere thanks to Aishwarya Trust for help in data collection.
Funding
Not applicable
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
Not applicable.
Ethics approval
Not applicable.
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human and animal rights
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The study is based on transplants done at Fortis Malar Hospital.
Rights and permissions
About this article

Cite this article
Balakrishnan, K., Nageswaran, C. Cost analysis of 163 consecutive heart transplant operationsin an Indian setting. Indian J Thorac Cardiovasc Surg 36 (Suppl 2), 200–209 (2020). https://doi.org/10.1007/s12055-020-00996-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-020-00996-z