
Abstract
Introduction
The role of multi detector computed tomography (MDCT) in thoracic trauma is continuously evolving with identification of occult injuries and better characterization of potentially life threatening injuries. Keeping this in mind, we have done a prospective study for volumetric analysis of lung parenchymal injury in isolated blunt thoracic trauma patients, explored its prognostic implications, and evaluated its correlation with clinical outcome of patient.
Methods
Prospective evaluation of patients with isolated blunt thoracic trauma coming from the trauma center was done with MDCT. Patients with poly trauma, pregnancy, penetrating thoracic trauma, pre-existing pulmonary or renal disease, and any other significant co-morbid medical or surgical illness and requirement of urgent thoracotomy (surgery) were excluded from the study. Data was collected regarding patient demographics, mechanism of injury, involvement of thoracic viscera and thoracic wall, uninvolved mean lung volume and overall prognosis in relation to eventless recovery, need for mechanical ventilation, and mortality which were taken as primary outcome parameters. Mean lung volumes of both lungs were compared in between groups of eventless recovery, need of mechanical ventilation and mortality with p value <0.05 considered to be significant.
Results
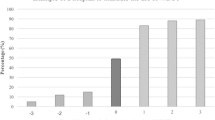
Sixty-two patients age range from 18 to 60 years, of blunt chest trauma were evaluated with MDCT after initial radiographs and the results were tabulated. The commonest mode of injury was motor vehicle accidents (74%). Overall mortality of thorax trauma-related death was 8% (five cases). Incidence of lung contusion was 90%, hemopneumothorax was 45%, rib fracture was 93%, cardiac injury was 1.6%, and diaphragmatic injury was 1.6%. Significant association (p < 0.05) of mortality and requirement for ventilation was found with remaining uninvolved mean volume of both lungs 1401.60±744.71 and 1676.00±360.31 cc respectively on volumetric analysis by MDCT 64-slice scan. Remaining uninvolved mean volume of both lungs 2645.00±609.57 cc on volumetric analysis by MDCT 64-slice scan was significantly associated (p < 0.05) with eventless recovery of patients.
Conclusion
Multi detector computed tomogram based calculation of uninvolved mean lung volumes following blunt thoracic trauma can help in determination of clinical outcome and requirement for mechanical ventilation. This study re-emphasizes the role of MDCT in thoracic trauma with providing help in better injury characterization and early assessment of prognostic implications. This information can act as guide to identify patients at high risk of complications, initiate early and aggressive kinetic chest therapy and explaining prognosis to patients or attendants. This study may also help in opening up other avenues for further research in thoracic trauma.





Similar content being viewed by others

References
Nirula R, Pintar FA. Identification of vehicle components associated with severe thoracic injury in motor vehicle crashes: a CIREN and NASS analysis. Accid Anal Prevo. 2008;40:137–41.
Devitt JH, Pagliarello G, Simons J. The involvement of anesthetists in critical care medicine. Can J Anaesth. 1990;37:S119.
Vodicka J, Spidlen V, Safranek J, Simanek V, Altmann P. Severe injury to the chest wall—experience with surgical therapy. Zentralbl Chir. 2007;132:542–6.
Warner KJ, Copass MK, Bulger EM. Paramedic use of needle thoracostomy in the prehospital environment. Prehosp Emerg Care. 2008;12:162–8.
Huber-Wagner S, Lefering R, Qvick LM, et al. Effect of whole-body CT during trauma resuscitation on survival: a retrospective, multicentre study. Lancet. 2009;373:1455–61.
Langdorf MI, Medak AJ, Hendey GW, et al. Prevalence and clinical import of thoracic injury identified by chest computed tomography but not chest radiography in blunt trauma: multicenter prospective cohort study. Ann Emerg Med. 2015;66:589–600.
De Knegt C, Meylaerts SA, Leenen LP. Applicability of the trimodal distribution of trauma deaths in a level I trauma centre in the Netherlands with a population of mainly blunt trauma. Injury. 2008;39:993–1000.
Miller PR, Croce MA, Bee TK, et al. ARDS after pulmonary contusion: accurate measurement of contusion volume identifies high-risk patients. Journal of Trauma-Injury Infection & Critical Care. 2001;51:223–30.
Wyen H, Wutzler S, Maegele M, et al. Rotational bed therapy after blunt chest trauma: a nationwide online-survey on current concepts of care in Germany. Injury. 2013;44:70–4.
Kaplan T, Atac GK, Gunal N, et al. Quantative computerized tomography assessment of lung density as a predictor of postoperative pulmonary morbidity in patients with lung cancer. J Thorac Dis. 2015;7:1391–7.
Iwano S, Okada T, Satake H, Naganawa S. 3D-CT volumetry of the lung using multidetector row CT: comparison with pulmonary function tests. Acad Radiol. 2009;16:250–6.
Wutzler S, Wafaisade A, Maegele M, et al. Lung organ failure score (LOFS): probability of severe pulmonary organ failure after multiple injuries including chest trauma. Injury. 2012;43:1507–12.
Watkins TR, Nathens AB, Cooke CR, et al. Acute respiratory distress syndrome after trauma: development and validation of a predictive model. Crit Care Med. 2012;40:2295–303. doi:10.1097/CCM.0b013e3182544f6a.
Reske AW, Reske AP, Heine T, et al. Computed tomographic assessment of lung weights in trauma patients with early posttraumatic lung dysfunction. Crit Care. 2011;15:R71.
Wicky S, Wintermark M, Schnyder P, Capasso P, Denys A. Imaging of blunt chest trauma. Eur Radiol. 2000;10:1524–38.
Liman ST, Kuzucu A, Tastepe AI, Ulasan GN, Topcu S. Chest injury due to blunt trauma. Eur J Cardiothorac Surg. 2003;23:374–8.
Tukralj I, Petrovic K, Stojanovi S, Petrovic D, Brakus A, Ristic J. Blunt chest trauma—an audit of injuries diagnosed by the MDCT examination. Vojnosanit Pregl. 2014;71:161–6. doi:10.2298/vsp1402161t.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
There was no funding for this study.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Pal, A.K., Kumar, S., Kumar, S. et al. Multi detector computed tomography based volumetric assessment of lung parenchymal injury in isolated blunt thoracic trauma patients acts as predictor of clinical outcome: a prospective observational study. Indian J Thorac Cardiovasc Surg 33, 213–219 (2017). https://doi.org/10.1007/s12055-017-0559-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-017-0559-1