
Abstract
Background
Chest trauma is a commonly encountered surgical emergency, constitutes about 10% of the total trauma, however 25% of fatalities are because of chest trauma. The aims of this study is to evaluate and document the causes modes of presentation, dignosis and modalities of treatment for chest trauma.
Patient and Methods
Prospetive study was done at Govt. Medical College (GMC) Jammu for a period of one year on cases of chest trauma. A total number of 2571 patients were admitted in Surgery department with poly trauma, 240 (9.3%) had chest injuries. Majority (78.7%) were males, with a mean age of 34.4 years. The mean hospital stay was 6.4 days and majority cases reached hospital with in 4 hours after injury. 81.7% cases had blunt trauma chest with Road Traffic Accidents (RTA) being the mode of injury and gunshot injury was the commonest among penetratting chest trauma victims. Clinical presentation and physical examination was sufficient for the dignosis, although some investigations, especially chest x-rays and thoracic Computed Tomographic (CT) scans were necessary in most of cases.
Observations
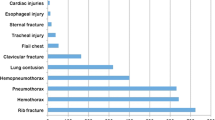
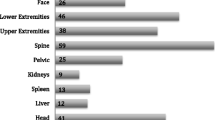
Only 16 (8.8%) patients required surgery and rest 91.2% managed on conservative line only. Rib fracture was the commonest injury (60%) followed by hemopneumothorax (51.7%), surgical emphysema (37.9), lung contusion (10.4%), flail chest (6.2%) etc. Associated injuries were seen in 117 (48.8%), with head injury the commonest one. Overall motality rate was 12%, which was higher in blunt chest trauma as compared to penetrating injuries. All these patients were managed by a protocol, which was standardized by postgraduate department of surgery of this institution.
Coclusion
The evaluation of thoracic injuries is important aspect of the total assessment of a severely injured patient, the incidence as high as 10%. Both diagnostic and therapeutic procedures go hand in hand most thoracic injuries can be treated adequately by intercostal tube drainage. Operative intervention has been found necessary in 6.75 of cases only
Similar content being viewed by others

References
Wisner D. Trauma to chest. Sabiston an Spencer WB Saunders publication 6th edition page 456; 1995.
Brathwaite CE, Rodriquez A, Turney SZ, Dunram CM, Cowey R. A 5-year experience. Blunt traumatic cardiac rupture. Ann Surg 1990; 212: 701–04.
Mandal AK, Oparah SS. Unusually low mortality of penetrating wounds of chest. Twelve years experience. J Thorac cardiovasc Surg 1989; 97: 119–25.
Sanidas E, Kefetzakis A, valassiadou K, Kassotakis G, Mihalakis J, Drasitis J, et al. Management of simple thoracic injuries at a level 1 trauma center: can primary health care center system take over. Injury 2000; 31: 669–75.
Zakharia AT Cardiovascular and thoracic battle injuries in the Lebanon war. Analysis of 3000 personal cases. J Thorac Cardiovasc Surg 1985; 89: 723–33.
LoCicero J 3rd, Mattox KL. Epidemology of chest trauma. Surg Clin North Am 1989; 69: 15–9.
Borlase BC, Metcalf RK, Moor EE, Manart FD. Penetrating wounds to the anterior chest. Analysis of thoracotomy and laparotomy. Am J Surg 1986; 152: 649–53.
Pate JW. Chest wall injuries. Surg Clinc North Am 1989; 69: 59–70.
Dulchasky SA, Hamilton DR, Diebel LN, Sargsyan AE, Billica RD, Williams DR. Thoractic ultrasound diagnosis of pneumothorax. J Trauma 1999; 47: 970–71.
Soldati G, Testa A, Silva FR Carbon L, Portale G, Silveri NG. Chest ultrasonography in lung contusion. Chest 2006; 130: 533–38.
Trupka A, Waydhas C, Hall feldt KK, Nast-Kolb D, Pfeifer KJ, Schweiberer. Value of thoracic computed tomography in the first assessment of severely injured patients with blunt chest trauma: Results of a Prospective study. J Trauma 1997; 43: 405–11.
Harrison WH, Gray AR, Couves CM, Howard JM. Severe non penetrating injuries to the chest. Clinical results in the management of 216 patients. Am J Surg 1960; 100: 715–22.
Ozgen G, Duygulu I, Solak H. Chest injuries in civilian life and their treatment. Chest 1984; 85: 89–92.
Richardson JD, Adamsl, Flint LM. Selective management of flail chest and pulmonary contusion. Ann Surg 1982; 196: 481–87.
Oparah SS, Mandal AK. Penetrating gunshot wounds of the chest in civilian practice: experience with 250 consecutive cases. Br J Surg 1978; 65: 45–48.
Van Way CW 3rd. Advanced techniques in thoracic trauma. Surg Clin North Am 1989; 69: 143–55.
Beall Ac Jr. Penetrating wounds of the aorta. Am J Surg 1960; 99: 770–74.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Atri, M., Singh, G. & Kohli, A. Chest trauma in Jammu region an institutional study. Indian J Thorac Cardiovasc Surg 22, 219–222 (2006). https://doi.org/10.1007/s12055-006-0006-1
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s12055-006-0006-1