
Abstract
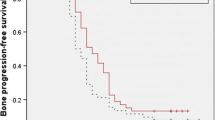
The aim of this study is to compare the efficacy and safety between zoledronic acid (ZA) and clodronate (CA) in the treatment of bone metastases for prostate cancer patients. We conducted a prospective study in recruiting 137 prostate cancer patients with bone metastases from 2008 to 2010. All men were well responding to first-line hormone therapy (PSA < 2 ng/mL); Patients were randomly assigned to receive zoledronic acid (4 mg over a 30 min infusion) every 1 month or to take 4 tablets per day of clodronate (1,600 mg) for up to 3 years. Bone mineral density (BMD) was measured by dual-energy X-ray absorptiometry at femoral neck, lumbar spine, and total hip, together with visual analog scale score were evaluated on baseline and 6, 12, 24, and 36 months, respectively. Toxicity and skeletal-related events (SREs) happened in both groups during this period were recorded down and compared. The ZA group had better bone progression-free survival (BPFS) (31 months vs 22 months, P = 0.04), but no statistical evidence of benefit was observed in terms of overall survival rate. The ZA group significantly increased lumbar spine BMD (4.5 ± 2.3 % vs CA group 2.3 ± 3.9 % P = 0.03), had a better response on pain-relieve effect (92 vs 76 % P = 0.002) and a rapid pain palliation (9 months vs 13 months P = 0.03). The CA group reported more gastrointestinal cases. However, the ZA group required more dose modifications. As compared to clodronate, Zoledronic acid has advantages on extending BPFS, better bone pain control and lumbar spine BMD performance for prostate cancer patients with bone metastases. The overall survival rate and SREs rate are similar.




Similar content being viewed by others


References
Yuen KK, Shelley M, Sze WM, Wilt T, Mason MD. Bisphosphonates for advanced prostate cancer. Cochrane Database Syst Rev. 2006;18(4):CD006250.
Coleman. Skeletal complications of malignancy. Cancer. 1997;80(8 Suppl):1588–94.
Rogers MJ, Gordon S, Benford HL, Coxon FP, Luckman SP, Monkkonen J, Frith JC. Cellular and molecular mechanisms of action of bisphosphonates. Cancer. 2004;88(12 Suppl):2961–78.
Aapro M, Abrahamsson PA, Body JJ, Coleman RE, Colomer R, Costa L, Crino L, Dirix L, Gnant M, Gralow J, Hadji P, Hortobagyi GN, Jonat W, Lipton A, Monnier A, Paterson AHG, Rizzoli R, Saad F, Thurlimann B. Guidance on the use of bisphosphonates in solid tumours: recommendations of an international expert panel. Ann Oncol. 2008;19(3):420–32.
Saad F. New research findings on zoledronic acid: survival, pain and anti-tumor effects. Cancer Treat Rev. 2008;34(2):183–92.
Dearnaley DP, Sydes MR, Mason MD, Stott M, Powell CS, Robinson AC, Thompson PM, Moffat LE, Naylor SL, Parmar MK, Mrc Pr05 Collaborators. A double-blind, placebo-controlled, randomized trial of oral sodium clodronate for metastatic prostate cancer (MRC PR05 Trial). J Natl Cancer Inst. 2003;95(17):1300–11.
Dearnaley DP, Mason MD, Parmar MK, Sanders K, Sydes MR. Adjuvant therapy with oral sodium clodronate in locally advanced and metastatic prostate cancer:long-term overall survival results from the MRC PR04 and MRC PR05 randomised controlled trials. Lancet Oncol. 2009;872–6. doi:10.1016/S1470-2045(09)70201-3.
Caraglia M, Santini D, Marra M, Vincenzi B, Tonini G, Budillon A. Emerging anti-cancer molecular mechanisms of aminobisphosphonates. Endocr Relat Cancer. 2006;13(1):7–26.
Yip SKH, Sim HG. Robotic radical prostatectomy in east Asia: development, surgical results and challenges. Curr Opin Urol. 2010;20(1):80–5. doi:10.1097/MOU.0b013e3283337bf0.
Kaufman JM, Johnell O, Abadie E, Adami S, Audran M, Avouac B, Sedrine WB, Calvo G, Devogelaer JP, Fuchs V, Kreutz G, Nilsson P, Pols H, Ringe J, Van Haelst L, Reginster JY. Background for studies on the treatment of male osteoporosis: state of the art. Ann Rheum Dis. 2000;59(10):765–72.
DePuy V, Anstrom KJ, Castel LD, Schulman KA, Weinfurt KP, Saad F. Effects of skeletal morbidities on longitudinal patient-reported outcomes and survival in patients with metastatic prostate cancer. Support Care Cancer. 2007;15(7):869–76.
Major PP, Cook R. Efficacy of bisphosphonates in the management of skeletal complications of bone metastases and selection of clinical endpoints. Am J Clin Oncol. 2002;25(6 Suppl 1):S10-8.
Lage MJ, Barber BL, Harrison DJ, Jun S. The cost of treating skeletal-related events in patients with prostate cancer. Am J Manag Care. 2008;14(5):317–22.
Sabry NA, Habib EE. Zoledronic acid and clodronate in the treatment of malignant bone metastases with hypercalcaemia; efficacy and safety comparative study. Med Oncol. 2011;28(2):584–90. doi:10.1007/s12032-010-9461-z.
Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L, Chin JL, Vinholes JJ, Goas JA, Chen B, Zoledronic Acid Prostate Cancer Study Group. A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94(19):1458–68.
Kanis JA, Johnell O, Oden A, Dawson A, De Laet C, Jonsson B. Ten year probabilities of osteoporotic fractures according to BMD and diagnostic thresholds. Osteoporos Int. 2001;12(12):989–95.
Faulkner KG. Bone matters: are density increases necessary to reduce fracture risk? J Bone Miner Res. 2000;15(2):183–7.
Rodrigues P, Hering FO, Bruna P, Meller A, Afonso Y. Comparative study of the protective effect of different intravenous bisphosphonates on the decrease in bone mineral density in patients submitted to radical prostatectomy undergoing androgen deprivation therapy. A prospective open-label controlled study. Int J Urol. 2007;14(4):317–20.
Yee CH, Ng CF, Wong AY, Chan CK, Hou SM, Yip SK. Zoledronic acid to prevent bone loss in Chinese men receiving androgen deprivation therapy for prostate cancer. Asia Pac J Clin Oncol. 2011;168–73. doi:10.1111/j.1743-7563.2011.01388.x.
Rosen LS, Gordon D, Tchekmedyian S, Yanagihara R, Hirsh V, Krzakowski M, Pawlicki M, de Souza P, Zheng M, Urbanowitz G, Reitsma D, Seaman JJ. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a Phase III, double-blind, randomized trial—the Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group. Clin Oncol. 2003;21(16):3150–7.
Rosen LS, Gordon D, Tchekmedyian NS, Yanagihara R, Hirsh V, Krzakowski M, Pawlicki M, De Souza P, Zheng M, Urbanowitz G, Reitsma D, Seaman J. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with non-small-cell lung carcinoma and other solid tumors: a randomized, Phase III, double-blind, placebo-controlled trial. Cancer. 2004;100(12):2613–21.
Agarwal MM, Khandelwal N, Mandal AK, Rana SV, Gupta V, Chandra Mohan V, Kishore GV. Factors affecting bone mineral density in patients with prostate carcinoma before and after orchidectomy. Cancer. 2005;103(10):2042–52.
Conde FA, Sarna L, Oka RK, Vredevoe DL, Rettig MB, Aronson WJ. Age, body mass index, and serum prostate-specific antigen correlate with bone loss in men with prostate cancer not receiving androgen deprivation therapy. Urology. 2004;64(2):335–40.
Ryan CW, Huo D, Stallings JW, Davis RL, Beer TM, McWhorter LT. Lifestyle factors and duration of androgen deprivation affect bone mineral density of patients with prostate cancer during first year of therapy. Urology. 2007;70(1):122–6.
Yakatan GJ, Poynor WJ, Talbert RL, Floyd BF, Slough CL, Ampulski RS, Benedict JJ. Clodronate kinetics and bioavailability. Clin pharmacol Ther. 1982;31(3):402–10.
Laitinen K, Patronen A, Harju P, Löyttyniemi E, Pylkkänen L, Kleimola T, Perttunen K. Timing of food intake has a marked effect on the bioavailability of clodronate. Bone. 2000;27(2):293–6.
Olson K, Van Poznak C. Significance and impact of bisphosphonate-induced acute phase responses. J Oncol Pharm Pract. 2007;13(4):223–9.
Acknowledgments
This study was funded by the Wenzhou science technology bureau (Y20100023). We thank lecturer Fengsu. Yang for her generous help in manuscript revision. This work has not been published in any other journal or publication.
Conflict of interest
All authors state that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, F., Chen, W., Chen, H. et al. Comparison between zoledronic acid and clodronate in the treatment of prostate cancer patients with bone metastases. Med Oncol 30, 657 (2013). https://doi.org/10.1007/s12032-013-0657-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12032-013-0657-x