
Abstract
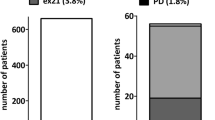
Erlotinib is a relatively well-tolerated treatment option for patients with advanced non-small-cell lung cancer (NSCLC). Some patients suffer from severe skin toxicity or diarrhea, making dose reductions or even treatment cessation necessary. Recent clinical trials usually defined a 100 mg daily dose as the lowest acceptable dose, whereas little is known about the efficacy with lower doses. We retrospectively reviewed the files of all patients with advanced non-small-cell lung cancer (NSCLC) treated with erlotinib. We assessed demographic, disease- and treatment-related information. We tried to correlate tolerability with clinical efficacy. EGF receptor exon 18/19/21 mutations were analyzed in selected patients. Fifty-three patients with advanced non-small-cell lung cancer were treated with erlotinib. In nine patients (17%), the doses had to be reduced to 75 or 50 mg daily due to toxicity. We observed several sustained disease stabilizations in this subgroup. Patients suffering from paronychia with erlotinib had a significantly longer time to progression than did subjects without nail toxicity (P = 0.04). If patients were free from any toxicity, they were at high risk for early tumor progression (P = 0.001) and death. In patients with disease stabilization for 6 months or longer, we observed EGFR 18/19/21 wild type, exon 19 and exon 21 mutations. In conclusion, several patients required dose reductions during treatment with erlotinib. However, in tumors with sensitivity to erlotinib, even daily doses of 50–75 mg can result in sustained disease control. Paronychia represents a favorable surrogate marker for efficacy.



Similar content being viewed by others

References
Pao W, et al. EGF receptor gene mutations are common in lung cancers from “never smokers” and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc Natl Acad Sci U S A. 2004;101:13306–11.
Jackman DM, et al. Exon 19 deletion mutations of epidermal growth factor receptor are associated with prolonged survival in non-small cell lung cancer patients treated with gefitinib or erlotinib. Clin Cancer Res. 2006;12:3908–14.
Riely GJ, et al. Clinical course of patients with non-small cell lung cancer and epidermal growth factor receptor exon 19 and exon 21 mutations treated with gefitinib or erlotinib. Clin Cancer Res. 2006;12:839–44.
Rosell R, et al. Screening for epidermal growth factor receptor mutations in lung cancer. N Engl J Med. 2009;361:958–67.
Cedres S, et al. Clinical surrogate markers of survival in advanced non-small cell lung cancer (NSCLC) patients treated with second-third line erlotinib. Lung Cancer. 2009;66:257–61.
Shepherd FA, et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med. 2005;353:123–32.
Reck M, et al. Erlotinib in Advanced non-small cell lung cancer: efficacy and safety findings of the global phase IV Tarceva lung cancer survival treatment study. J Thorac Oncol. 2010;5:1616–22.
Tiseo M, et al. An expanded access program of erlotinib (Tarceva) in patients with advanced non-small cell lung cancer (NSCLC): data report from Italy. Lung Cancer. 2009;64:199–206.
Lind JS, et al. Dramatic response to low-dose erlotinib of epidermal growth factor receptor mutation-positive recurrent non-small cell lung cancer after severe cutaneous toxicity. J Thorac Oncol. 2009;4:1585–6.
Yeo WL, et al. Erlotinib at a dose of 25 mg daily for non-small cell lung cancers with EGFR mutations. J Thorac Oncol. 2010;5:1048–53.
Conflict of interest
Dr Binder received travel expenses and congress registration fees from Roche Pharma AG.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Binder, D., Buckendahl, AC., Hübner, RH. et al. Erlotinib in patients with advanced non-small-cell lung cancer: impact of dose reductions and a novel surrogate marker. Med Oncol 29, 193–198 (2012). https://doi.org/10.1007/s12032-010-9767-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12032-010-9767-x