
Abstract
Background
Predictions of functional outcome in neurocritical care (NCC) patients impact care decisions. This study compared the predictive values (PVs) of good and poor functional outcome among health care providers with and without NCC training.
Methods
Consecutive patients who were intubated for ≥ 72 h with primary neurological illness or neurological complications were prospectively enrolled and followed for 6-month functional outcome. Medical intensive care unit (MICU) attendings, NCC attendings, residents (RES), and nurses (RN) predicted 6-month functional outcome on the modified Rankin scale (mRS). The primary objective was to compare these four groups’ PVs of a good (mRS score 0–3) and a poor (mRS score 4–6) outcome prediction.
Results
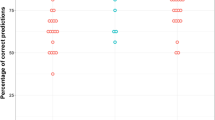
Two hundred eighty-nine patients were enrolled. One hundred seventy-six had mRS scores predicted by a provider from each group and were included in the primary outcome analysis. At 6 months, 54 (31%) patients had good outcome and 122 (69%) had poor outcome. Compared with other providers, NCC attendings expected better outcomes (p < 0.001). Consequently, the PV of a poor outcome prediction by NCC attendings was higher (96% [95% confidence interval [CI] 89–99%]) than that by MICU attendings (88% [95% CI 80–93%]), RES (82% [95% CI 74–88%]), and RN (85% [95% CI 77–91%]) (p = 0.047, 0.002, and 0.012, respectively). When patients who had withdrawal of life-sustaining therapy (n = 67) were excluded, NCC attendings remained better at predicting poor outcome (NCC 90% [95% CI 75–97%] vs. MICU 73% [95% CI 59–84%], p = 0.064). The PV of a good outcome prediction was similar among groups (MICU 65% [95% CI 52–76%], NCC 63% [95% CI 51–73%], RES 71% [95% CI 55–84%], and RN 64% [95% CI 50–76%]).
Conclusions
Neurointensivists expected better outcomes than other providers and were better at predicting poor functional outcomes. The PV of a good outcome prediction was modest among all providers.

Similar content being viewed by others


References
Society of Critical Care Medicine. Critical Care Statistics. https://www.sccm.org/Communications/Critical-Care-Statistics Accessed Jan 31, 2021.
Barrett ML, Smith MW, Elixhauser A, Honigman LS, Pines JM. Utilization of Intensive Care Services, 2011. HCUP Statistical Brief #185. December 2014. Agency for Healthcare Research and Quality, Rockville, MD. https://hcup-us.ahrq.gov/reports/statbriefs/sb185-Hospital-Intensive-Care-Units-2011.jsp (copy and paste) Accessed Jan 31, 2021.
Hemphill JC III, Bonovich DC, Besmertis L, et al. The ICH Score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32:891–7.
Hemphill JC III, Farrant M, Neill TA. Prospective validation of the ICH score for 12-month functional outcome. Neurology. 2009;73:1088–94.
Zahuranec DB, Lisabeth LD, Sánchez BN, et al. Intracerebral hemorrhage mortality is not changing despite declining incidence. Neurology. 2014;82:2180–6.
Gadhia R, McCane D, Lee J, Ling KC, Jiang K, Chui D. The HOPES registry-Houston methodist hospital outcomes-based prospective endpoints in stroke. J Stroke Cerebrovasc Dis. 2018;27:2973–6.
Albers GW, Marks MP, Kemp S, et al. Thrombectomy for stroke at 6–16 hours with selection by perfusion imaging. N Engl J Med. 2018;378:708–18.
Sculier C, Gainza-Lein M, Fernandez IS, Loddenkemper T. Long-term outcomes of status epilepticus: a critical assessment. Epilepsia. 2018;59(Suppl 2):155–69.
Cook D, Rocker G, Marshall J, et al. Withdraw of mechanical ventilation in anticipation of death in the intensive care unit. N Engl J Med. 2003;349:1123–32.
Diringer M, Edwards D, Aiyagari V, Hollingsworth H. Factors associated with withdrawal of mechanical ventilation in the neurology/neurosurgery intensive care unit. Crit Care Med. 2001;29:1792–7.
Smith AK, White DB, Arnold RM. Uncertainty-the other side of prognosis. N Engl J Med. 2013;368(26):2448–50.
Finley Caulfield A, Gabler L, Lansberg MG, et al. Outcome prediction in mechanically ventilated neurologic patients by junior neurointensivists. Neurology. 2010;74:1096–101.
Hwang DY, Dell CA, Sparks MJ, et al. Clinician judgement versus formal scales for predicting intracerebral hemorrhage outcomes. Neurology. 2016;86:126–33.
Chu SY, Hwang DY. Predicting outcome for intracerebral hemorrhage patients: current tools and their limitations. Semin Neurol. 2016;36:254–60.
van Swieten JC, Koudstaal PJ, Visser MC, Shouten HJ, van Gijn J. Inter-observer agreement for the assessment of handicap in stroke patients. Stroke. 1988;19:604–7.
Lopez-Cancio E, Salvat M, Cerda N, et al. Phone and video-based modalities of central blinded adjudication of modified rankin scores in an endovascular stroke trial. Stroke. 2015;46:3405–10.
Wilson JTL, Pettigrew LEL, Teasdale GM. Structural interviews for the Glasgow outcome scale and the extended Glasgow outcome scale: guidelines for their use. J Neurotrauma. 1998;15:573–85.
Pettigrew LEL, Wilson JTL, Teasdale GM. Reliability of ratings on the Glasgow outcome scales from in-person and telephone structured interviews. J Head Trauma Rehabil. 2003;18:252–8.
Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–5.
Korner-Bitensky N, Wood-Dauphinee S. Barthel index information elicited over the telephone. Is it reliable? Am J Phys Med Rehabil. 1995;74:9–18.
Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. New Engl J Med. 2005;352:777–85.
Vahedi K, Hofmeijer J, Juettler E, et al. Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomized controlled trials. Lancet Neurol. 2007;6:215–22.
Vahedi K, Vicant E, Mateo J, et al. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL Trial). Stroke. 2007;38:2506–17.
Juttler E, Schwab S, Schmiedek P, et al. Decompressive surgery for the treatment of malignant infarction of the middle cerebral artery (DESTINY): a randomized, controlled trial. Stroke. 2007;38:2518–25.
Hofmeijer J, Kapelle LJ, Algra A, et al. Surgical decompression for space-occupying cerebral infarction (the hemicraniectomy after middle cerebral artery infarction with life-threatening edema trial [HAMLET]): a multicenter, open, randomized trial. Lancet Neurol. 2009;8:326–33.
Berkhemer OA, Fransen PSS, Beurmer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20.
van den Berg LA, Dijkgraaf MGW, Berkhemer OA, et al. Two-year outcome after endovascular treatment for acute ischemic stroke. N Engl J Med. 2017;376:1341–9.
Qureshi AI, Palesch YY, Barsan WG, et al. for the ATACH-2 Trial investigators and the neurological emergency treatment trials network. Intensive blood-pressure lowering in patients with acute cerebral hemorrhage. N Engl J Med. 2016;375:1033–43.
Hanley DF, Lane K, McBee N, et al. for the CLEAR III Investigators. Thrombolytic removal of intraventricular haemorrhage in treatment of severe stroke: results of the randomized, multicenter, multiregional, placebo-controlled CLEAR II trial. Lancet 2017; 389:603–611.
Hanley DF, Thompson RE, Rosenblum M, et al. Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): a randomized, controlled, open-label, blinded endpoint phase 3 trial. Lancet. 2019;393:1021–32.
Witsch J, Frey HP, Patel S, et al. Prognostication of long-term outcomes after subarachnoid hemorrhage: the FRESH score. Ann Neurol. 2016;80:46–58.
Creutzfeldt CJ, Halloway RG. Treatment decisions after severe stroke – uncertainty and biases. Stroke. 2012;43:3405–8.
Albrecht GL, Devlieger PJ. The disability paradox: high quality of life against all odds. Soc Sci Med. 1999;48:977–88.
Saposnik G, Cote R, Mamdani M, et al. JURaSSiC Accuracy of clinician versus risk score prediction of ischemic stroke outcomes. Neurology. 2013;81:448–55.
Becker KJ, Baxter AB, Cohen WA, et al. Withdrawal of support in intracerebral hemorrhage may lead to self-fulfilling prophecies. Neurology. 2001;56(6):766-772.25.
Hemphill JC III, Newman J, Zhao S, Johnston SC. Hospital usage of early do-not-resuscitate orders and outcome after intracerebral hemorrhage. Stroke. 2004;35(5):1130–4.
Zahuranec DB, Brown DL, Lisabeth LD, et al. Early care limitations independently predict mortality after intracerebral hemorrhage. Neurology. 2007;68(20):1651–7.
Silvennoinen K, Meretoja A, Strbian D, Putaala J, Kaste M, Tatlisumak T. Do-not-resuscitate (DNR) orders in patients with intracerebral hemorrhage. Int J Stroke. 2014;9(1):53–8.
Creutzfeldt CJ, Becker KJ, Weinstein JR, et al. Do-not-attempt resuscitation orders and prognostic models for intraparenchymal hemorrhage. Crit Care Med. 2011;39(1):158–62.
Morgenstern LB, Zahuranec DB, Sánchez BN, et al. Full medical support for intracerebral hemorrhage. Neurology. 2015;84(17):1739–44.
Hemphill JC III, Greenberg SM, Anderson CS, et al. AHA/ASA Guidelines for the management of spontaneous intracerebral hemorrhage. Stroke. 2015;46:2032–60.
Kiphuth IC, Köhrmann M, Lichy C, Schwab S, Huttner HB. Hemicraniectomy for malignant middle cerebral artery infarction: retrospective consent to decompressive surgery depends on functional long-term outcome. Neurocrit Care. 2010;13:380–4.
Zier LS, Burack JH, Micco G, et al. Doubt and belief in physicians’ ability to prognosticate during critical illness: the perspective of surrogate decision makers. Crit Care Med. 2008;36:2341–7.
Acknowledgements
The authors would like to acknowledge the following contributors and organizations: (1) Christine A. C. Wijman, MD, PhD (deceased 2013), who was involved in the study design and initial data analysis; (2) the Program in Organizing Neuroethics Education and Research (PIONEAR), Stanford University (2006-2007); (3) the Stanford critical care medicine team and nurses; and (4) our patients and their families.
Funding
Anna Finley Caulfield reports receiving past funding (2006–2007) from the Program in Organizing Neuroethics Education and Research (PIONEAR), Stanford University. Maarten G. Lansberg reports receiving past funding (2005–2006) from the Stanford Bio-X grant.
Author information
Authors and Affiliations
Contributions
Anna Finley Caulfield design and the conceptualized study, analyzed the data, and drafted the manuscript for intellectual content. Michael Mlynash interpreted the data, analyzed the data, conducted the statistical analysis, and revised the manuscript for intellectual content. Irina Eyngorn contributed a major role in the acquisition of data. Maarten Lansberg designed and the conceptualized study, interpreted the data, and revised the manuscript for intellectual content. Anousheh Afjei contributed a major role in the acquisition of data. Chitra Venkatasubramanian interpreted the data and revised the manuscript for intellectual content. Marion Buckwalter interpreted the data and revised the manuscript for intellectual content. Karen Hirsch interpreted the data and revised the manuscript for intellectual content. The final manuscript was approved by all authors.
Corresponding author
Ethics declarations
Conflicts of interest
The authors report no disclosures relevant to the article.
Ethical approval/informed consent
This study was approved by the Stanford Institutional Review Boad.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Finley Caulfield, A., Mlynash, M., Eyngorn, I. et al. Prognostication of ICU Patients by Providers with and without Neurocritical Care Training. Neurocrit Care 37, 190–199 (2022). https://doi.org/10.1007/s12028-022-01467-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-022-01467-6