
Abstract
Background
In aneurysmal subarachnoid hemorrhage (aSAH), one of the main determinants of prognosis is delayed cerebral ischemia (DCI). Transcranial Doppler (TCD) is used to monitor vasospasm and DCI. We aimed to better understand cerebral hemodynamics response to hypertension induction (HI) with norepinephrine (NE) and inotropic therapy with milrinone so that TCD can be a bedside tool in helping to guide DCI therapies. Our primary objective was to determine TCD blood flow velocity (BFV) kinetics during HI and inotropic therapy for DCI treatment. Secondly, we performed an analysis by treatment subgroups and evaluated clinical response to therapies.
Methods
We performed a prospective observational cohort study in a Brazilian high-volume center for aSAH. Patients with aSAH admitted between 2016 and 2018 who received NE or milrinone for DCI treatment were included. TCDs were performed before therapy initiation (t0) and 45 (t1) and 90 min (t2) from the onset of therapy. For each DCI event, we analyzed the highest mean flow velocity (MFV) and the mean MFV and compared their kinetics over time. The National Institutes of Health Stroke Scale was determined at t0, t1, and t2.
Results
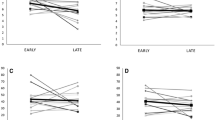
Ninety-eight patients with aSAH were admitted during the study period. Twenty-one (21.4%) developed DCI, of whom six had DCI twice, leading to a total of 27 analyzed DCI events (12 treated with HI and 15 with milrinone). Patients treated with NE had their mean arterial pressure raised (85 mm Hg in t0, 112 mm Hg in t2 [p < 0.001]), whereas those treated with milrinone had a significant decrease in mean arterial pressure over treatment (94 mm Hg in t0, 88 mm Hg in t2 [p = 0.004]). Among all treated patients, there was a significant drop from t0 to t2 but not to t1 in the highest MFV and in the highest mean MFV. Among those treated with HI, there were no significant changes from t0 to t1 or t2 (highest MFV in t0 163.2 cm/s, in t1 172.9 cm/s [p = 0.27], and in t2 164 cm/s [p = 0.936]). Conversely, in those treated with milrinone, there was a significant decrease from t0 to t1 and to t2 (highest MFV in t0 197.1 cm/s, in t1 172.8 cm/s [p = 0.012], in t2 159 cm/s [p = 0.002]). Regarding clinical outcomes, we observed a significant improvement in mean National Institutes of Health Stroke Scale scores from 17 to 16 in t1 (p < 0.001) and to 15 in t2 (p = 0.002).
Conclusions
BFV analyzed by TCD in patients with aSAH who developed DCI and were treated with milrinone or NE significantly decreased in a time-dependent way. Milrinone effectively decrease cerebral BFV, whereas NE do not. Clinical improvement was achieved with both treatment strategies.



Similar content being viewed by others


References
Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJ. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 2009;8(7):635–42.
de Oliveira Manoel AL, Goffi A, Marotta TR, Schweizer TA, Abrahamson S, Macdonald RL. The critical care management of poor-grade subarachnoid haemorrhage. Crit Care. 2016;20:21.
Lawton MT, Vates GE. Subarachnoid hemorrhage. N Engl J Med. 2017;377(3):257–66.
Vergouwen MD, Vermeulen M, van Gijn J, Rinkel GJ, Wijdicks EF, Muizelaar JP, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. 2010;41(10):2391–5.
Macdonald RL. History and definition of delayed cerebral ischemia. Acta Neurochir Suppl. 2013;115:3–7.
Cossu G, Messerer M, Oddo M, Daniel RT. To look beyond vasospasm in aneurysmal subarachnoid haemorrhage. Biomed Res Int. 2014;628587:1–1.
Budohoski KP, Guilfoyle M, Helmy A, Huuskonen T, Czosnyka M, Kirollos R, et al. The pathophysiology and treatment of delayed cerebral ischaemia following subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 2014;85(12):1343–53.
Oliveira Manoel AL, Mansur A, Murphy A, Turkel-Parrella D, MacDonald M, MacDonald RL, et al. Aneurysmal subarachnoid haemorrhage from a neuroimaging perspective. Crit Care. 2014;18(6):557.
Sloan MA, Alexandrov AV, Tegeler CH, Spencer MP, Caplan LR, Feldmann E, et al. Assessment: transcranial Doppler ultrasonography: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2004;62(9):1468–81.
Lysakowski C, Walder B, Constanza MC, Tremer MR. Transcranial doppler versus angiography in patients with vasospasm due to a ruptured cerebral aneurysm: a systematic review. Stroke. 2001;32:2292–8.
Francoeur CL, Mayer SA. Management of delayed cerebral ischemia after subarachnoid hemorrhage. Crit Care. 2016;20(1):277.
de Oliveira Manoel AL, Turkel-Parrella D, Duggal A, Murphy A, McCredie V, Marotta TR. Managing aneurysmal subarachnoid hemorrhage: it takes a team. Cleve Clin J Med. 2015;82(3):177–92.
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43(6):1711–37
Diringer MN, Bleck TP, Claude Hemphill J 3rd, Menon D, Shutter L, Vespa P, et al. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocrit Care. 2011;15(2):211–40.
Rouanet C, Silva GS. Aneurysmal subarachnoid hemorrhage: current concepts and updates. Arq Neuropsiquiatr. 2019;77(11):806–14.
Dankbaar JW, Slooter AJ, Rinkel GJ, Schaaf IC. Effect of different components of triple-H therapy on cerebral perfusion in patients with aneurysmal subarachnoid haemorrhage: a systematic review. Crit Care. 2010;14(1):R23.
Lannes M, Zeiler F, Guichon C, Teitelbaum J. The use of milrinone in patients with delayed cerebral ischemia following subarachnoid hemorrhage: A systematic review. Can J Neurol Sci. 2017;44(2):152–60.
Venkatraman A, Khawaja AM, Gupta S, Hardas S, Deveikis JP, Harrigan MR, et al. Intra-arterial vasodilators for vasospasm following aneurysmal subarachnoid hemorrhage: a meta-analysis. J Neurointerv Surg. 2018;10(4):380–7.
Muehlschlegel S, Rordorf G, Bodock M, Sims JR. Dantrolene mediates vasorelaxation in cerebral vasoconstriction: a case series. Neurocrit Care. 2009;10(1):116–21.
Muehlschlegel S, Rordorf G, Sims J. Effects of a single dose of dantrolene in patients with cerebral vasospasm after subarachnoid hemorrhage: a prospective pilot study. Stroke. 2011;42(5):1301–6.
Daftari Besheli L, Tan CO, Bell DL, Hirsch JA, Gupta R. Temporal evolution of vasospasm and clinical outcome after intra-arterial vasodilator therapy in patients with aneurysmal subarachnoid hemorrhage. PLoS ONE. 2017;12(3):e0174676.
Lannes M, Teitelbaum J, del Pilar CM, Cardoso M, Angle M. Milrinone and homeostasis to treat cerebral vasospasm associated with subarachnoid hemorrhage: the Montreal Neurological Hospital Protocol. Neurocrit Care. 2012;16(3):354–62.
Froese L, Dian J, Gomez A, Unger B, Zeiler FA. The cerebrovascular response to neropineprhine: a scoping systematic review of the animal and human literature. Pharmacol Res Perspect. 2020;8(5):e00655. https://doi.org/10.1002/prp2.655.
Gathier CS, Dankbaar JW, van der Jagt M, Verweji BH, Oldenbeuving AW, Rinkel GJ, et al. Effects of induced hypertension on cerebral perfusion in delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: a randomized clinical trial. Stroke. 2015;46(11):3277–81.
Kim DH, Joseph M, Ziadi S, Nates J, Dannenbaium M, et al. Increase in cardiac output can reverse flow deficits from vasospasm independent of blood pressure: a study using xenon computed tomographic measurement of cerebral blood flow. Neurosurgery. 2003;53:1044–52.
Soliman R, Zohry G. Effect of magnesium sulphate and milrinone on cerebral vasospasm after aneurysmal subarachnoid hemorrhage: a randomized study. Rev Bras Anestesiol. 2019;69(1):64–71.
Alamri AS, Alturki A, Badawy M, Letourneau J, Lannes M, Angle M, et al. Safety and outcome of high doses IV milirinone in subarachnoid hemorrhage with refractory vasospasm. Stroke. 2016;47:ATM101–ATM101.
Haegens NM, Gathier CS, Horn J, Coert BA, Verbaan D, van den Bergh WM. Induced hypertension in preventing cerebral infarction in delayed cerebral ischemia after subarachnoid hemorrhage. Stroke. 2018;49(11):2630–6.
de Oliveira Manoel AL, Mansur A, Silva GS, Germans MR, Jaja BNR, Kouzmina E, et al. Functional outcome after poor-grade subarachnoid hemorrhage: a single-center study and systematic literature review. Neurocrit Care. 2016;25(3):338–50.
Gathier CS, van den Bergh WM, van der Jagt M, Verweij BH, Dankbaar JW, Muller MC, et al. Induced hypertension for delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: a randomized clinical trial. Stroke. 2018;49(1):76–83.
Otsubo H, Takemae T, Inoue T, Kobayashi S, Sugita K. Normovolaemic induced hypertension therapy for cerebral vasospasm after subarachnoid haemorrhage. Acta Neurochir. 1990;103:18–26.
Lasry O, Marcoux J. The use of intravenous milrinone to treat cerebral vasospasm following traumatic subarachnoid haemorrhage. Springerplus. 2014;3:633.
Funding
This study received no funding.
Author information
Authors and Affiliations
Contributions
All authors contributed equally to this work.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflicts.
Ethical approval/informed consent
The current study has been approved by the appropriate institutional and national research ethics committee and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent has been provided by all participants of this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rouanet, C., Chaddad, F., Freitas, F. et al. Kinetics of cerebral blood flow velocities during treatment for delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage. Neurocrit Care 36, 226–239 (2022). https://doi.org/10.1007/s12028-021-01288-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-021-01288-z