
Abstract
Introduction
In patients with aneurysmal subarachnoid hemorrhage (aSAH), it is unclear whether aneurysm treatment <24 h after ictus results in better outcomes than treatment 24–72 h after aSAH. We studied whether aneurysm occlusion <24 h is associated with better outcomes than occlusion 24–72 h after aSAH.
Methods
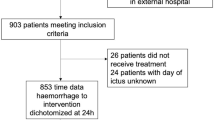
We used two cohorts of patients with aSAH: (1) the UMC Utrecht cohort with patients admitted between 2008 and 2012 and (2) the International Subarachnoid Aneurysm Trial cohort. Aneurysm treatment was categorized into <24 h and 24–72 h after ictus. We calculated adjusted risk ratios (aRRs) with 95 % confidence intervals (CIs) using Poisson regression analyses for poor functional outcome (death or dependency) for both cohorts separately, and performed a pooled analysis based on individual patient data. We also performed a worst-case scenario analysis wherein all patients with rebleeding >3 h after admission were re-categorized into the group with aneurysm treatment 24–72 h after aSAH.
Results
We included 1,238 patients (UMC Utrecht cohort: n = 330; ISAT: n = 908). The aRR for poor outcome after treatment <24 h was in the UMC Utrecht cohort 1.84 (95 % CI: 1.25-2.70), in ISAT 1.14 (95 % CI 0.84–1.55), in the pooled analysis 1.37 (95 % CI 1.11–1.68), and in the worst-case scenario pooled analysis 1.24 (95 % CI 1.01–1.52).
Conclusion
Our results suggest that aneurysm occlusion can be performed in day time within 72 h after ictus, instead of on an emergency basis. However, due to the retrospective, non-randomized design of our study, our results cannot be considered as definitive evidence.




Similar content being viewed by others

References
Ohman J, Heiskanen O. Timing of operation for ruptured supratentorial aneurysms: a prospective randomized study. J Neurosurg. 1989;70:55–60.
Steiner T, Juvela S, Unterberg A, Jung C, Forsting M, Rinkel G, European Stroke Organization. European Stroke Organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrhage. Cerebrovasc Dis. 2013;35:93–112.
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, American Heart Association Stroke Council, Council on Cardiovascular Radiology and Intervention, Council on Cardiovascular Nursing, Council on Cardiovascular Surgery and Anesthesia, Council on Clinical Cardiology, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43:1711–37.
Brilstra EH, Rinkel GJ, Algra A, van Gijn J. Rebleeding, secondary ischemia, and timing of operation in patients with subarachnoid hemorrhage. Neurology. 2000;55:1656–60.
Cronqvist M, Wirestam R, Ramgren B, Brandt L, Nilsson O, Saveland H, et al. Diffusion and perfusion MRI in patients with ruptured and unruptured intracranial aneurysms treated by endovascular coiling: complications, procedural results, MR findings and clinical outcome. J Neuroradiol. 2005;47:855–73.
Grunwald IQ, Papanagiotou P, Politi M, Struffert T, Roth C, Reith W. Endovascular treatment of unruptured intracranial aneurysms: occurrence of thromboembolic events. J Neurosurg. 2006;58:612–8.
Hahnemann ML, Ringelstein A, Sandalcioglu IE, Goericke S, Moenninghoff C, Wanke I, et al. Silent embolism after stent-assisted coiling of cerebral aneurysms: diffusion-weighted MRI study of 75 cases. J Neurointerv Surg. 2013;. doi:10.1136/neurintsurg-2013-010820.
Kang DH, Kim BM, Kim DJ, Suh SH, Kim DI, Kim YS, et al. MR-DWI-positive lesions and symptomatic ischemic complications after coiling of unruptured intracranial aneurysms. Stroke. 2013;44:789–91.
Soeda A, Sakai N, Murao K, Sakai H, Ihara K, Yamada N, et al. Thromboembolic events associated with Guglielmi detachable coil embolization with use of diffusion-weighted MR imaging. Part II. Detection of the microemboli proximal to cerebral aneurysm. AJNR Am J Neuroradiol. 2003;24:2035–8.
Teasdale GM, Drake CG, Hunt W, Kassell N, Sano K, Pertuiset B, et al. A universal subarachnoid hemorrhage scale: report of a committee of the World Federation of Neurosurgical Societies. J Neurol Neurosurg Psychiatry. 1988;51:1457.
Jennett B, Teasdale G, Braakman R, Minderhoud J, Knill-Jones R. Predicting outcome in individual patients after severe head injury. Lancet. 1976;1:1031–4.
Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 2002;360:1267–74.
Vergouwen MD, Vermeulen M, van Gijn J, Rinkel GJ, Wijdicks EF, Muizelaar JP, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. 2010;41:2391–5.
Dorhout Mees SM, Kerr RS, Rinkel GJ, Algra A, Molyneux AJ. Occurrence and impact of delayed cerebral ischemia after coiling and after clipping in the International Subarachnoid Aneurysm Trial (ISAT). J Neurol. 2012;259:679–83.
van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1988;19:604–7.
Phillips TJ, Dowling RJ, Yan B, Laidlaw JD, Mitchell PJ. Does treatment of ruptured intracranial aneurysms within 24 hours improve clinical outcome? Stroke. 2011;42:1936–45.
Wong GK, Boet R, Ng SC, Chan MT, Gin T, Zee B, et al. Ultra-early (within 24 hours) aneurysm treatment after subarachnoid hemorrhage. World Neurosurg. 2012;77:311–5.
Sandström N, Yan B, Dowling R, Laidlaw J, Mitchell P. Comparison of microsurgery and endovascular treatment on clinical outcome following poor-grade subarachnoid hemorrhage. J Clin Neurosci. 2013;20:1213–8.
Gu DQ, Zhang X, Luo B, Long XA, Duan CZ. Impact of ultra-early coiling on clinical outcome after aneurysmal subarachnoid hemorrhage in elderly patients. Acad Radiol. 2012;19:3–7.
Sehba FA, Hou J, Pluta RM, Zhang JH. The importance of early brain injury after subarachnoid hemorrhage. Prog Neurobiol. 2012;97:14–37.
Sehba FA, Mostafa G, Knopman J, Friedrich V Jr, Bederson JB. Acute alterations in microvascular basal lamina after subarachnoid hemorrhage. J Neurosurg. 2004;101:633–40.
Sehba FA, Mostafa G, Friedrich V Jr, Bederson JB. Acute microvascular platelet aggregation after subarachnoid hemorrhage. J Neurosurg. 2005;102:1094–100.
Bederson JB, Levy AL, Ding WH, Kahn R, DiPerna CA, Jenkins AL III, et al. Acute vasoconstriction after subarachnoid hemorrhage. J Neurosurg. 1998;42:352–62.
Claassen J, Carhuapoma JR, Kreiter KT, Du EY, Connolly ES, Mayer SA. Global cerebral edema after subarachnoid hemorrhage: frequency, predictors, and impact on outcome. Stroke. 2002;33:1225–32.
Acknowledgments
None.
Funding
None.
Conflict of interest
Andrew Molyneux reports a consulting agreement with Sequent Medical Inc. All other authors have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oudshoorn, S.C., Rinkel, G.J.E., Molyneux, A.J. et al. Aneurysm Treatment <24 Versus 24–72 h After Subarachnoid Hemorrhage. Neurocrit Care 21, 4–13 (2014). https://doi.org/10.1007/s12028-014-9969-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-014-9969-8