
Abstract
Background
To date, common therapy in patients with intracranial hemorrhage (ICH) includes prophylaxis of seizure using antiepileptic drugs, commonly phenytoin. Phenytoin therapy is associated with a high incidence of cognitive disturbance. Levetiracetam is known to cause less cognitive disruption and may be a suitable alternative for seizure prophylaxis. Cognitive outcomes in ICH patients receiving seizure prophylaxis with levetiracetam or phenytoin are compared.
Method
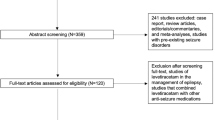
A retrospective chart review was conducted with 269 patients who received prophylactic levetiracetam or phenytoin between August 2005 and May 2008. A total of 85 reviewed patients met inclusion criteria (phenytoin n = 25, levetiracetam n = 60).
Results
Statistically significant results included higher Glasgow Coma Scores (GCS) at dismissal (median, 14 vs. 11, P = 0.023), lower seizure incidence (0.0 vs. 8%, P = 0.03) for patients receiving levetiracetam than those treated with phenytoin and patients being discharged home (21.7% vs. 16%, P = 0.03). Observed trends included greater cognitive function retention rate (56.7% vs. 36%, P = 0.08).
Conclusion
Despite similarities in hemorrhage type and severity at onset, patients receiving levetiracetam had better cognition at discharge and fewer seizures than patients receiving phenytoin. These data suggest that levetiracetam is more effective than phenytoin for seizure prophylaxis without suppression of cognitive abilities in patients with ICH.


Similar content being viewed by others


References
Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics–2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119(3):e21–181.
Hart R, Byer J, Slaughter J, Hewett J, Easton J. Occurrence and implications of seizures in subarachnoid hemorrhage due to ruptured intracranial aneurysms. Neurosurgery. 1981;8(4):417–21.
Keränen T, Tapaninaho A, Hernesniemi J, Vapalahti M. Late epilepsy after aneurysm operations. Neurosurgery. 1985;17(6):897–900.
Kotila M, Waltimo O. Epilepsy after stroke. Epilepsia. 1992;33(3):495–8.
Olafsson E, Gudmundsson G, Hauser W. Risk of epilepsy in long-term survivors of surgery for aneurysmal subarachnoid hemorrhage: a population-based study in Iceland. Epilepsia. 2000;41(9):1201–5.
Ryvlin P, Montavont A, Nighoghossian N. Optimizing therapy of seizures in stroke patients. Neurology. 2006;67(12 Suppl 4):S3–9.
Chumnanvej S, Dunn I, Kim D. Three-day phenytoin prophylaxis is adequate after subarachnoid hemorrhage. Neurosurgery. 2007;60(1):99–102. (discussion 102–103).
Choudhari K, Kaliaperumal C. Three-day phenytoin prophylaxis is adequate after subarachnoid hemorrhage. Neurosurgery. 2007;61(6):E1340. (author reply E1340).
Zubkov A, Wijdicks E. Antiepileptic drugs in aneurysmal subarachnoid hemorrhage. Rev Neurol Dis. 2008;5(4):178–81.
Carpay J, Aldenkamp A, van Donselaar C. Complaints associated with the use of antiepileptic drugs: results from a community-based study. Seizure. 2005;14(3):198–206.
Naidech A, Kreiter K, Janjua N, et al. Phenytoin exposure is associated with functional and cognitive disability after subarachnoid hemorrhage. Stroke. 2005;36(3):583–7.
Díaz R, Sancho J, Serratosa J. Antiepileptic drug interactions. Neurologist. 2008;14(6 Suppl 1):S55–65.
Rogawski M. Diverse mechanisms of antiepileptic drugs in the development pipeline. Epilepsy Res. 2006;69(3):273–94.
Arif H, Buchsbaum R, Weintraub D, Pierro J, Resor SJ, Hirsch L. Patient-reported cognitive side effects of antiepileptic drugs: predictors and comparison of all commonly used antiepileptic drugs. Epilepsy Behav. 2009;14(1):202–9.
Nau K, Divertie G, Valentino A, Freeman W. Safety and efficacy of levetiracetam for critically ill patients with seizures. Neurocrit Care. 2009;11(1):34–7.
Szaflarski J, Meckler J, Szaflarski M, Shutter L, Privitera M, Yates S. Levetiracetam use in critically ill patients. Neurocrit Care. 2007;7(2):140–7.
Lynch B, Lambeng N, Nocka K, et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc Natl Acad Sci USA. 2004;101(26):9861–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Taylor, S., Heinrichs, R.J., Janzen, J.M. et al. Levetiracetam is Associated with Improved Cognitive Outcome for Patients with Intracranial Hemorrhage. Neurocrit Care 15, 80–84 (2011). https://doi.org/10.1007/s12028-010-9341-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-010-9341-6