
Abstract
Introduction Hyponatremia frequently complicates acute brain injury and may precipitate neurological worsening by promoting cerebral edema. An increase in brain water may be better managed through water excretion than with fluid restriction or hypertonic fluids. Vasopressin-receptor antagonists such as conivaptan, which promote free water excretion, may be ideal agents to treat this common and potentially serious disorder.
Methods The efficacy of intermittent bolus doses of conivaptan to correct hyponatremia was examined in a consecutive series of patients treated in our neurointensive care unit. Patients were excluded if baseline sodium was over 135 mEq/l or if another conivaptan dose was given within 12 h. We assessed the proportion responding with a 4 or 6 mEq/l rise in sodium by 12 h, the change in sodium from baseline, and, in those not receiving another dose for at least 72 h, the long-term ability of a single dose to maintain sodium at least 4 mEq/l above baseline. We also recorded the effects of conivaptan on urine output and specific gravity, and noted any adverse events.
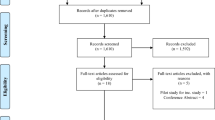
Results A total of 25 doses given to 19 patients were included (out of 44 total doses administered in the study period). Sodium rose by 5.8 ± 3.2 mEq/l within 12 h, with 71% rising by at least 4 mEq/l and 52% manifesting at least a 6 mEq/l increase. In those receiving only a single dose, 69% maintained at least a 4 mEq/l rise up to 72 h. Conivaptan also consistently led to increased urine output and a significant drop in urine specific gravity (i.e., aquaresis). No cases of phlebitis were observed despite administration of conivaptan through peripheral IVs.
Conclusion Intermittent dosing of conivaptan was effective in increasing free water excretion and correcting hyponatremia in neurologically ill patients. This supports its further evaluation for managing hyponatremia in this population.


Similar content being viewed by others


References
Lester MC, Nelson PB. Neurological aspects of vasopressin release and the syndrome of inappropriate secretion of antidiuretic hormone. Neurosurgery. 1981;8(6):735–40. doi:10.1097/00006123-198106000-00020.
Doczi T, Tarjanyi J, Huszka E, Kiss J. Syndrome of inappropriate secretion of antidiuretic hormone after head injury. Neurosurgery. 1982;10(6 Pt 1):685–8.
Qureshi AI, Suri MF, Sung GY, et al. Prognostic significance of hypernatremia and hyponatremia among patients with aneurysmal subarachnoid hemorrhage. Neurosurgery. 2002;50(4):749–55. doi:10.1097/00006123-200204000-00012.
Rabinstein AA, Wijdicks EF. Hyponatremia in critically ill neurological patients. Neurologist. 2003;9(6):290–300. doi:10.1097/01.nrl.0000095258.07720.89.
Multz AS. Vasopressin dysregulation and hyponatremia in hospitalized patients. J Intensive Care Med. 2007;22(4):216–23. doi:10.1177/0885066607301360.
Pasantes-Morales H, Lezama RA, Ramos-Mandujano G, Tuz KL. Mechanisms of cell volume regulation in hypo-osmolality. Am J Med. 2006;119(Suppl 1(7)):S4–11. doi:10.1016/j.amjmed.2006.05.002.
Gullans SR, Verbalis JG. Control of brain volume during hyperosmolar and hypoosmolar conditions. Annu Rev Med. 1993;44:289–301. doi:10.1146/annurev.me.44.020193.001445.
Bhardwaj A. Neurological impact of vasopressin dysregulation and hyponatremia. Ann Neurol. 2006;59(2):229–36. doi:10.1002/ana.20788.
Fraser CL, Arieff AI. Epidemiology, pathophysiology, and management of hyponatremic encephalopathy. Am J Med. 1997;102(1):67–77. doi:10.1016/S0002-9343(96)00274-4.
Diringer MN, Zazulia AR. Hyponatremia in neurologic patients: consequences and approaches to treatment. Neurologist. 2006;12(3):117–26. doi:10.1097/01.nrl.0000215741.01699.77.
Singhi SC, Singhi PD, Srinivas B, et al. Fluid restriction does not improve the outcome of acute meningitis. Pediatr Infect Dis J. 1995;14(6):495–503. doi:10.1097/00006454-199506000-00006.
Wijdicks EF, Vermeulen M, Hijdra A, van Gijn J. Hyponatremia and cerebral infarction in patients with ruptured intracranial aneurysms: is fluid restriction harmful? Ann Neurol. 1985;17(2):137–40. doi:10.1002/ana.410170206.
Gross P, Reimann D, Henschkowski J, Damian M. Treatment of severe hyponatremia: conventional and novel aspects. J Am Soc Nephrol. 2001;12(Suppl 17):S10–4.
Mohmand HK, Issa D, Ahmad Z, Cappuccio JD, Kouides RW, Sterns RH. Hypertonic saline for hyponatremia: risk of inadvertent overcorrection. Clin J Am Soc Nephrol. 2007;2(6):1110–7. doi:10.2215/CJN.00910207.
Woo MH, Kale-Pradhan PB. Fludrocortisone in the treatment of subarachnoid hemorrhage-induced hyponatremia. Ann Pharmacother. 1997;31(5):637–9.
Wijdicks EF, Vermeulen M, van Brummelen P, van Gijn J. The effect of fludrocortisone acetate on plasma volume and natriuresis in patients with aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 1988;90(3):209–14. doi:10.1016/0303-8467(88)90023-6.
Porzio P, Halberthal M, Bohn D, Halperin ML. Treatment of acute hyponatremia: ensuring the excretion of a predictable amount of electrolyte-free water. Crit Care Med. 2000;28(6):1905–10. doi:10.1097/00003246-200006000-00037.
Cawley MJ. Hyponatremia: current treatment strategies and the role of vasopressin antagonists. Ann Pharmacother. 2007;41(5):840–50. doi:10.1345/aph.1H502.
Hays RM. Vasopressin antagonists––progress and promise. N Engl J Med. 2006;355(20):2146–8. doi:10.1056/NEJMe068236.
Palm C, Pistrosch F, Herbrig K, Gross P. Vasopressin antagonists as aquaretic agents for the treatment of hyponatremia. Am J Med. 2006;119(Suppl 1(7)):S87–92. doi:10.1016/j.amjmed.2006.05.014.
Rabinstein AA. Vasopressin antagonism: potential impact on neurologic disease. Clin Neuropharmacol. 2006;29(2):87–93. doi:10.1097/00002826-200603000-00006.
Zeltser D, Rosansky S, van Rensburg H, Verbalis JG, Smith N. Assessment of the efficacy and safety of intravenous conivaptan in euvolemic and hypervolemic hyponatremia. Am J Nephrol. 2007;27(5):447–57. doi:10.1159/000106456.
Ghali JK, Koren MJ, Taylor JR, et al. Efficacy and safety of oral conivaptan: a V1A/V2 vasopressin receptor antagonist, assessed in a randomized, placebo-controlled trial in patients with euvolemic or hypervolemic hyponatremia. J Clin Endocrinol Metab. 2006;91(6):2145–52. doi:10.1210/jc.2005-2287.
Vaprisol (conivaptan hydrochloride injection). Prescribing information. Deerfield Ill: Astellas Pharma US, Inc.; 2007.
Burnier M, Fricker AF, Hayoz D, Nussberger J, Brunner HR. Pharmacokinetic and pharmacodynamic effects of YM087, a combined V1/V2 vasopressin receptor antagonist in normal subjects. Eur J Clin Pharmacol. 1999;55(9):633–7. doi:10.1007/s002280050685.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Murphy, T., Dhar, R. & Diringer, M. Conivaptan Bolus Dosing for the Correction of Hyponatremia in the Neurointensive Care Unit. Neurocrit Care 11, 14–19 (2009). https://doi.org/10.1007/s12028-008-9179-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-008-9179-3