
Abstract
Objective
Gonadal and sexual disturbances are commonly encountered in patients with Cushing’s disease. Nevertheless, the prevalence of hypogonadism in male Cushing’s disease, the risk factors as well as the recovery time have been scarcely reported. Therefore, we aimed to explore the prevalence of hypogonadism at baseline and its determinants. In addition, the recovery time of hypogonadism and risk factors for unrecovered gonadal axis in male Cushing’s disease with biochemical remission were investigated.
Methods
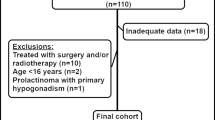
We reviewed medical records of males with Cushing’s disease managed between 2010 and 2020. Fifty-two male patients were enrolled according to the criteria. Each case attained biochemical remission after transsphenoidal surgery. Demographic details, clinical features, 24-hour UFC, hormonal profile [serum PRL, FSH, LH, TT, ACTH, cortisol, TT4/FT4, TT3/ FT3, TSH and IGF-1] were measured at baseline and during follow-up. The maximal tumor diameter on MRI was recorded at diagnosis.
Results
Hypogonadotropic hypogonadism was observed in thirty-nine patients (75%) at diagnosis. Total testosterone was negatively correlated with ACTH and 24-hour UFC. Midnight serum ACTH level at diagnosis was significantly associated with hypogonadism after adjusting for confounding factors. Thirty-two (80%) patients achieved eugonadism within 12 months after the surgery, of which twenty-eight (87.5%) achieved eugonadism within 3 months. Seven patients were persistently hypogonadal during the follow-up (≥1 year), mainly due to the hypopituitarism as a complication of the therapies such as surgery.
Conclusion
Hypogonadotropic hypogonadism is frequent in male Cushing’s disease, but it is reversible in most cases within one-year follow-up after remission.




Similar content being viewed by others


Data availability
The data analyzed during the study are not publicly available due to relevant regulations, but are available from corresponding authors on reasonable request.
Abbreviations
- UFC:
-
urinary free cortisol;
- PRL:
-
prolactin;
- FSH:
-
follicle-stimulating hormone;
- LH:
-
luteinizing hormone;
- TT:
-
total testosterone;
- ACTH:
-
adrenocorticotrophic hormone;
- TT4:
-
total thyroxine;
- FT4:
-
free thyroxine;
- TT3:
-
total triiodothyronine;
- FT3:
-
free triiodothyronine;
- TSH:
-
thyroid-stimulating hormone;
- IGF-1:
-
insulin-like growth factor 1;
- HH:
-
hypogonadotropic hypogonadism;
- BMI:
-
body mass index.
References
A.G. Smals, P.W. Kloppenborg, T.J. Benraad, Plasma testosterone profiles in Cushing’s syndrome. J. Clin. Endocrinol. Metab. 45(2), 240–245 (1977)
J.P. Luton, P. Thieblot, J.C. Valcke, J.A. Mahoudeau, H. Bricaire, Reversible gonadotropin deficiency in male Cushing’s disease. J. Clin. Endocrinol. Metab. 45(3), 488–495 (1977)
M. Fleseriu, R.J. Auchus, I. Bancos, A. Ben-Shlomo, J. Bertherat, N.R. Biermasz, C.L. Boguszewski, M.D. Bronstein, M. Buchfelder, J.D. Carmichael et al. Consensus on diagnosis and management of Cushing’s disease: a guideline update. Lancet Diabetes Endocrinol. 9(12), 847–875 (2021)
M. Fleseriu, I.A. Hashim, N. Karavitaki, S. Melmed, M.H. Murad, R. Salvatori, M.H. Samuels, Hormonal replacement in hypopituitarism in adults: an endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 101(11), 3888–3921 (2016)
A. Dutta, N. Gupta, R. Walia, A. Bhansali, P. Dutta, S.K. Bhadada, R. Pivonello, C.K. Ahuja, S. Dhandapani, A. Hajela et al. Remission in Cushing’s disease is predicted by cortisol burden and its withdrawal following pituitary surgery. J. Endocrinol. Invest. 44(9), 1869–1878 (2021)
Chinese Pituitary Adenoma Cooperative Group, Consensus of Chinese experts on diagnosis and treatment of Cushing’s disease. Natl. Med. J. China 96(11), 835–840 (2016)
E.V. Varlamov, G. Vila, M. Fleseriu, Perioperative management of a patient with cushing disease. J. Endocr. Soc. 6(3), bvac010 (2022)
L.K. Nieman, B.M. Biller, J.W. Findling, M.H. Murad, J. Newell-Price, M.O. Savage, A. Tabarin; Endocrine Society, Treatment of cushing’s syndrome: an endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 100(8), 2807–2831 (2015)
M.D. Hurtado, T. Cortes, N. Natt, W.F. Young Jr, I. Bancos, Extensive clinical experience: Hypothalamic-pituitary-adrenal axis recovery after adrenalectomy for corticotropin-independent cortisol excess. Clin. Endocrinol. (Oxf) 89(6), 721–733 (2018)
S. Shekhar, S. Gubbi, R. McGlotten, L. Nieman, SAT-459 Hypothalamic-Pituitary-Gonadal (HPG) and Hypothalamic-Pituitary-Thyroid (HPT) axes in Cushing Syndrome (CS): a retrospective cohort study. J. Endocrine Soc 3(Suppl 1), SAT-459 (2019).
Acknowledgements
The authors are indebted to the patients who participated in this study and all the doctors contributing to the diagnosis and treatment of these patients.
Author information
Authors and Affiliations
Contributions
H.P.Z. and Q.W. analyzed the data and wrote the manuscript. Q.Y.S., Q.L.C., W.W. and L.J.J. collected the data. Z.Y.M., M.S., X.F.S., Y.F.W. and Y.Z. performed transsphenoidal surgeries. Y.M.L. and Z.Y.Z. revised the study and manuscript. B.L. and M.H. recruited patients. H.Y.Y. and S.Z. conducted the study design and quality control. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zheng, H., Wang, Q., Cui, Q. et al. The hypothalamic-pituitary-gonad axis in male Cushing’s disease before and after curative surgery. Endocrine 77, 357–362 (2022). https://doi.org/10.1007/s12020-022-03083-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-022-03083-y