
Abstract
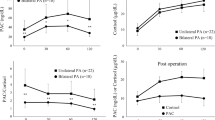
Incidentally discovered adrenal masses are diagnosed with increasing frequency, especially among patients with hypertension. Thus, a reliable screening test for primary hyperaldosteronism (PA) is essential to avoid unnecessary diagnostic procedures to this population. The aim of the present study is the evaluation of aldosterone to renin ratio (ARR), using plasma renin concentration, in the diagnostic algorithm of patients with adrenal incidentaloma. A total of 123 individuals were studied: 17 patients with proven PA (age 55.5 ± 1.4 years), 27 patients with nonfunctioning adrenal incidentaloma (age 60.3 ± 1.8 years, 14 hypertensives and 13 normotensives) and 79 control subjects (age 58.7 ± 1.4 years, 27 hypertensives and 52 normotensives). A receiver operating characteristic (ROC) analysis disclosed that an ARR ≥32 combines a sensitivity of 100% with a specificity of 96.2% for the diagnosis of PA. No difference in ΑRR between hypertensive and normotensive individuals harbouring an adrenal incidentaloma and hypertensive and normotensive controls was found. Patients with adrenal incidentalomas with subtle glucocorticoid hypersecretion demonstrated similar ARR compared to patients with normal cortisol secretion. In conclusion, ARR is reliable for the exclusion of PA in patients with adrenal incidentalomas. Furthermore, subtle aldosterone hypersecretion, as indicated by increased ARR, in patients with adrenal incidentalomas is not associated with the presence of hypertension or subtle glucocorticoid hypersecretion.




Similar content being viewed by others

References
M.M. Grumbach, B.M. Biller, G.D. Braunstein, K.K. Campbell, J.A. Carney, P.A. Godley, E.L. Harris, J.K. Lee, Y.C. Oertel, M.C. Posner, J.A. Schlechte, H.S. Wieand, Management of the clinically inapparent adrenal mass (“incidentaloma”) [NIH Conference]. Ann. Inter. Med. 138, 424–429 (2003)
G. Mansmann, J. Lau, E. Balk, M. Rothberg, Y. Miyachi, S.R. Bornstein, The Clinically Inapparent Adrenal Mass: Update in Diagnosis and management. Endocr. Rev. 25, 309–340 (2004)
F. Mantero, M. Terzolo, G. Arnaldi, G. Osella, A.M. Masini, A. Ali, M. Giovagnetti, G. Opocher, A. Angeli, A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology. J. Clin. Endocrinol. Metab. 85, 637–644 (2000)
G. Bernini, A. Moretti, G. Argenio, A. Salvetti, Primary aldosteronism in normokalemic patients with adrenal incidentalomas. Eur. J. Endocrinol. 146, 523–529 (2002)
W.F. Young, (2007). The incidentally discovered adrenal mass. N. Engl. J. Med. 356, 601–610
S. Tsagarakis, C. Roboti, P. Kokkoris, V. Vasiliou, C. Alevizaki, N.C. Thalassinos, Elevated post dexamethasone suppression cortisol concentrations correlate with hormonal alterations of the hypothalamo-pituitary adrenal axis in patients with adrenal incidentalomas. Clin. Endocrinol. 49, 165–171 (1998)
N. Valli, B. Catargi, N. Ronci, V. Vergnot, F. Leccia, J.M. Ferriere, G. Chene, N. Grenier, F. Laurent, A. Tabarin, Biochemical screening for subclinical cortisol-secreting adenomas amongst adrenal incidentalomas. Eur. J. Endocrinol. 144, 401–408 (2001)
W.F. Young, Primary hyperaldosteronism: renaissance of a syndrome. Clin. Endocrinol. 66, 607–618 (2007)
K. Hiramatsu, T. Yamada, Y. Yukimura, I. Komiya, K. Ichikawa, M. Ishihara, H. Nagata, T. Izumiyama, A screening test to identify aldosterone producing adenoma by measuring plasma renin activity: results in hypertensive patients. Arch. Inter. Med. 141, 1589–1593 (1981)
N.M. Kaplan, The current epidemic of primary aldosteronism: causes and consequences. J. Hypertens. 22, 863–869 (2004)
R.D. Gordon, The challenge of more robust and reproducible methodology in screening for primary aldosteronism. J. Hypertens. 22, 251–255 (2004)
J.K. Doig, K.S. Lees, J.L. Reid, The effect of drugs on the renin-angiotensin system in man. in The Renin-angiotensin System, eds. by J.I.S. Robertson, M.G. Nicholls (Merk, London, 1993), pp. 80.1–80.19
T.J. McKenna, S.J. Sequeira, A. Heffernan, J. Chambers, S. Cunningham, Diagnosis under random conditions of all disorders of the renin-angiotensin-aldosterone axis, including primary hyperaldosteronism. J. Clin. Endocrinol. Metabol. 73, 952–957 (1991)
A. Tanabe, M. Naruse, S. Takagi, K. Tsuchiya, T. Imaki, K. Takano, Variability in the renin/aldosterone profile under random and standardized sampling conditions in primary aldosteronism. J. Clin. Endocrinol. Metabol. 88, 2489–2494 (2003)
S.J. Duffy, E.S. Biegelsen, R.T. Eberhardt, D.F. Kahn, B.A. Kingwell, J.A. Vita, Low-renin hypertension with relative aldosterone excess is associated with impaired NO-mediated vasodilation. Hypertension 46, 707–713 (2005)
S.C. Tiu, C.H. Choi, C.C. Shek, Y.w. Ng, F.K.W. Chan, C.M. Ng, A.P. Kong, The use of aldosterone-renin ratio as a diagnostic test for primary hyperaldosteronism and its test characteristics under different conditions of blood sampling. J. Clin. Endocrinol. Metabol. 90, 72–78 (2005)
P.E. Plouin, P. Cudek, J.F. Arnal, T.T. Guyene, P. Corvol, Immunoradiometric assay of active renin versus determinations of plasma renin activity in the clinical investigation of hypertension, congestive heart failure, and liver cirrhosis. Horm. Res. 34, 138–141 (1990)
F.H. Derkx, C. Steuknkel, M.P. Schalckamp, W. Visser, I.H. Huisveld, M.A. Schalckamp, Immunoreactive renin, prorenin and enzymatically active renin in plasma during pregnancy, and in women taking oral contraceptives. J. Clin. Endocrinol. Metabol. 63, 1008–1015 (1986)
C.E. Fardella, L. Mosso, C. Gomez-Sanchez, P. Cortes, J. Soto, L. Gómez, M. Pinto, A. Huete, E. Oestreicher, A. Foradori, J. Monterol, Primary hyperaldosteronism in essential hypertensives: prevalence, biochemical profile, and molecular biology. J. Clin. Endocrinol. Metabol. 85, 1863–1867. (2000)
G.W. Liddle, Tests of pituitary-adrenal suppressability in the diagnosis of Cushing’s syndrome. J. Clin. Endocrinol. Metabol. 20, 1539–1560 (1960)
J.A. Hanley, B.I. Mc Neil, The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 143, 29–36 (1982)
P. Mulatero, F. Rabbia, A. Milan, C. Paglieri, F. Morello, L. Chiandussi, F. Veglio, Drug effects on Aldosterone/Plasma Renin Activity ratio in primary aldosteronism. Hypertention 40, 897–902 (2002)
C. Scifarth, S. Trenkel, H. Schobel, E.G. Hahn, J. Hensen, Influence of antihypertensive medication on aldosterone and renin concentration on in the differential diagnosis of essential hypertension and primary aldosteronism. Clin Endocrinol. 57, 457–465 (2002)
N. Unger, I.L. Schmidt, C. Pitt, M.K. Walz, T. Philipp, K. Mann, S. Petersenn, Comparison of active renin concentration and plasma renin activity for the diagnosis of primary hyperaldosteronism in patients with adrenal mass. Eur. J. Endocrinol. 150, 517–523 (2004), (a) P. Mulatero et al., Trends Endocrinol. Metab. 16,114–119 (2005)
P. Mulatero, M. Stowasser, K.F. Loh, C.E. Fardella, R.D. Gordon, L. Mosso, C.E. Gomez-Sanchez, F. Veglio, W.E. Young, Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J. Clin. Endocrinol. Metabol. 154, 865–873 (2004)
D.A. Calhoun, M.K. Nishizaka, M.A. Zaman, R.B. Thakkar, P. Weissmann, Hyperaldosteronism among black and white subjects with resistant hypertension. Hypertension 40, 892–896 (2002)
W.F. Young Jr Minireview: primary aldosteronism––changing concepts in diagnosis and treatment. Endocrinol. 144, 2208–2213 (2003)
J.S. Williams, G.H. Williams, A. Raji, X. Jeunemaitre, N.J. Brownv P.N. Hopkins, P.R. Conlin, Prevalence of primary hyperaldosteronism in mild to moderate hypertension without hypokalaemia. J. Hum. Hypertens. 20, 129–136. (2006)
C. Schirpenbach, L. Seiler, C. Maser-Gluth, F. Rudiger, C. Nickel, F. Beuschlein, Confirmatory testing in normokalaemic primary aldosteronism. Eur. J. Endocrinol. 154, 865–873 (2006)
P. Mulatero, A. Milan, F. Fallo, G. Regolisti, F. Pizzolo, C. Fardella, L. Mosso, L. Marafetti, F. Veglio, M. Maccario, Comparison of confirmatory tests for the diagnosis of primary aldosteronism. J. Clin. Endocrinol. Metabol. 91, 2618–2623. (2006)
P. Mulatero, R.G. Dluhy, G. Giacchetti, M. Boscaro, F. Veglio, P. Stiewart, Diagnosis of primary aldosteronism: from screening to subtype differentiation. Trends Endocrinol. Metab. 16, 114–119 (2005)
M. Terzolo, A. Pia, A. Ali, G. Osella, G. Reimondo, S. Bovio, F. Daffara, M. Procopio, P. Paccotti, G. Borretta, A. Angeli, Adrenal incidentaloma: a new cause of the metabolic syndrome? J. Clin. Endocrinol. Metabol. 87, 998–1003. (2002)
S. Tsagarakis, D. Vassiliadi, N. Thalassinos, Endogenous subclinical hypercortisolism: diagnostic uncertainties and clinical implications. J. Endocrinol. Invest. 29, 471–82. (2006)
J. Adachi, Y. Hirai, K. Terui, T. Nakano, Y. Fukuda, T. Suda, H. Sasano, Report of 7 Cases of Adrenal Tumors Secreting Both Cortisol and Aldosterone Internal Medicine, vol. 42. (2003) pp. 714–718
T. Saito, A. Ikoma, T. Saito, H. Tamemoto, Y. Suminaga, S. Yamada, M. Kawakami, T. Suzuki, H. Sasano, S.E. Ishikawa, Possibly simultaneous primary aldosteronism and preclinical Cushing’s syndrome in a patient with double adenomas of right adrenal gland. Endocr. J. 54, 287–93 (2007)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tzanela, M., Effremidis, G., Vassiliadi, D. et al. The aldosterone to renin ratio in the evaluation of patients with incidentally detected adrenal masses. Endocr 32, 136–142 (2007). https://doi.org/10.1007/s12020-007-9028-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-007-9028-8