
Abstract
Mineral imbalance in the body may significantly contribute to the development and course of hypertension. In this paper, blood pressure figures have been linked to the levels of Fe, Ca, Mg, Zn, Cu, Na and K in hair. The research sample was composed of young men (n = 91) aged 13–21, from the town of Mafinga, Iringa District, Tanzania. The data collected included their age, tribal background and weekly diet. Based on body mass index, the participants were categorised into pre-defined subgroups. To examine how the minerals in question affect blood pressure, correlation analysis and multiple ridge regression analysis were performed. Analysis of ridge regression findings for the researched group (n = 91) shows that the minerals under scrutiny account for systolic blood pressure variation in 13 % and in 15 % for diastolic blood pressure variation. After including two additional variables—calendar age and body mass index—in regression analysis, the ultimate coefficient of determination (R 2) changes for systolic blood pressure and remains the same for diastolic blood pressure (R 2 = 0.194 and R 2 = 0.156, respectively). Nutritional analysis shows that the students included in the study received insufficient calories per day (1,500–2,200 kcal). The group of students with abnormal blood pressure were not aware of their poor health. Research findings may result from progressive environmental changes and poor nutrition in terms of food quantity and quality, which had an impact on the subjects’ blood pressure. Hair analysis used to determine mineral content in the body may be an auxiliary tool in identifying the links between factors leading to the development of hypertension.
Similar content being viewed by others

Introduction
Hypertension is a condition with a multi-factor pathogenesis. Epidemiological studies have found links between high blood pressure and age, sex, race, geographic location, local industrialisation level, lifestyle, nutrition and work [1–6]. Studies of blood pressure among Africans in their native countries also emphasise ethnic, cultural and genetic diversity. An important role is played by socio-cultural factors and living conditions which determine nutrition in terms of quantity and quality. The last two factors seem to be directly responsible for the levels of individual minerals in the human body. Their contents and participation in fundamental metabolic processes in living organisms have been recognised quite well, yet there is no consensus regarding the optimum levels of individual minerals for a human being. It is believed that mineral imbalance may significantly contribute to the development and course of hypertension [7–10].
Population studies in Africa are seriously hindered by socio-economic factors and their consequences [11]. The living conditions determine the supply of minerals in the daily diet, and the diet affects the mineral content in the body. These associations are analysed in hypertension studies, too. Other important factors include drinking water, degree of food processing [12, 13] and individual capacity for mineral absorption. Research methods and techniques, which make it possible to determine the physiologically optimal health, are subject to continuous verification [14]. What changes is not only the definition of what is considered to be the optimal level of a given mineral in a living human body [15] but also our knowledge on the areas and force of influence exerted by minerals on the living organism. It is vital that minerals are present in the human body in specific concentrations. Mineral deficiency or excess may lead to serious metabolic disorders, impair immune processes and cause various complications and illnesses, or even lead to death. It is considered that abnormal levels of Na and K in the body are the strongest determinants in inducing arterial hypertension. A linear dependence was found between the Na levels in the body and 24-h blood pressure results. The Na/K ratio in the body is also an important indicator [7–10, 16]. Potassium, calcium and magnesium homeostases are closely related. Hypokalaemia and hypocalcaemia are frequent finding in patients with hypomagnesaemia, and both predict the presence of hypomagnesaemia. There is an inverse relationship between Mg intake and blood pressure, and epidemiological studies show an increased incidence of hypertension in areas where the Mg content in water is low [17]. Zn concentration in the diet plays an important role in the regulation of systolic blood pressure and can be a critical nutrient for maintenance of anti-oxidative events in spontaneously hypertensive rats [18]. Synergistic and antagonistic interactions between minerals disturbed proportions—all these affect concentration levels of other minerals and may, for instance, have considerable impact on the development of arterial hypertension.
Blood pressure in the human body is not a static value. It can be affected by many factors [16, 19, 20]. Three key factors may be identified, which affect mineral levels in the human body:
-
Quantities deriving from the environment
-
Individual needs of the body
-
Mineral absorption and elimination capacity of the body.
In this paper, blood pressure levels are assessed in combination with concentration levels of Fe, Ca, Mg, Zn, Cu, Na and K in the hair of young men of the Bantu language group, from the town of Mafinga, Tanzania.
Materials and Methods
Material to be used in the analysis of hair mineral levels came from young men (n = 91) aged 13–21, secondary school students from the town of Mafinga, Iringa District, Tanzania. Mafinga lies at 2,300 m a.s.l. latitude (DMS) 7°15′ 0 S and longitude (DMS) 35°4′ 0E.
Anthropological examination included measurements of body height (B-v) and weight. The questionnaire section collected information on tribal background, place of permanent residence of the subjects and their parents, medical history, type and quantity of food and whether the subject was (or had been) a tobacco smoker. They all belonged to the Bantu language group, and they were all staying at the school boarding house and ate meals at the school canteen.
Blood pressure was measured at the left wrist using an oscillometric device, the electronic blood pressure monitor BRAUN BP 3560 (type 6085). The device indicated whether the arm was kept in the right position (at heart level) during the measurement. The blood pressure monitor was equipped with a cuff adjusting to wrist length (13.5–20 cm). The accuracy rate of this device is ±3 mm Hg. Examinations were conducted from morning till noon, at room temperature, before physical exertion in a relaxed sitting position. Arterial hypertension criteria were defined at ≥140 mm Hg for systolic blood pressure (SBP) and/or ≥90 mm Hg for diastolic blood pressure (DBP). The adopted thresholds are consistent with the guidelines of the World Health Organisation (WHO) [6, 21]. The blood pressure monitor was also used to measure the resting heart rate (HR) per minute.
Body height measurements (B-v) were made with an anthropometer, in compliance with the anthropometric technique [22], while body weight was measured using SOEHNLE electronic weighing scales, with an accuracy of within 100 g. All examinations were voluntary and not invasive, and the students signed up for measurements willingly.
The body mass index was calculated (BMI = kg/m2), and on this basis, the subjects were classified into categories [23]. The BMI of the studied young men helped determine whether the problem of excess weight was present in the group and to what extent body mass could affect the blood pressure results in the individuals examined.
Analysis of the Content of Chemical Elements in Hair
Hair samples were obtained from people who did not have coloured or treated hair. Samples (50–100 mg) were collected from the nape of the neck, as in Rębacz et al. [24]. Briefly, the hair was placed in ultrasonic bath of distilled deionised water (Milli-Q purification system, Millipore) for 1 h. Thereafter, washed twice using acetone and allowed to dry overnight in laminar flow hood at 25 °C. Hair was digested in a Teflon vessel with 1 mL of 65 % HNO3, 1 mL of 70 % HClO4. The samples were then left to solve for 48 h in laminar flow hood at 25 °C. Thereafter, the samples were subject to 30 min mineralization using a BM-1S/II microwave mineraliser (Plazmotronika, Wrocław, Poland). The samples was evaporated to dryness in N2, and its residue was taken up in 10 % HNO3 to volume of 5 mL distilled deionised water. Concentrations of Fe, Ca, Mg, Zn and Cu were analysed by atomic absorption spectrometry (PU 9100X, Philips) in air-acetylene flame, calibrated with standard solutions (Merck, Germany). The calibration curve was determined automatically by the computer connected to the spectrometer. The determination was carried out in an air-acetylene flame with lamps of the following wave lengths: Ca, 422.7 nm (0.5 % solution of lanthanum was added as a buffer solution); Mg, 285.2 nm (0.1 % solution of lanthanum or strontium was added as a buffer); Fe, 248.3 nm; Zn, 213.9 nm; and Cu, 324.7 nm. Concentration of Na and K was measured by flame emission spectroscopy method using an atomic absorption spectrometer (PU 9100X, Philips). Concentrations were read from the curve traced on the basis of Titrisol standards by Merck. For sodium, a 589.0-nm wavelength was used, and for potassium, 766.5 nm was used. In determining sodium levels, 0.2 % potassium solution was used as ionisation buffer and determinations were made in oxygen-acetylene flame. Potassium determinations were made in nitrous suboxide-acetylene flame. Control assays were carried out every 10 samples. The coefficients of variation were as follows: Fe, 9 %; Ca, 9 %; Zn, 8 %; Cu, 9 %; Mg, 9 %, Na, 5 %; and K, 5 %.
On the basis of SBP and/or DBP, subgroups were identified of young men with high blood pressure in both measurements and those in whom either SBP or DBP exceeded the normal range. The collected material was compiled and is presented herein in table format (Table 1, 2, 3, 4, 5, 6, 7, 8, 9, 10 and 11). To examine how the minerals in question affect blood pressure, correlation analysis and multiple ridge regression analysis were performed. The application of the latter method seems the most fitting. It allows for a comprehensive assessment of how the explanatory variables included in the model influence SBP and DBP. The classic version of the multiple regression analysis is sensitive to situations where explanatory variables are correlated not only with each other but also with the explained variable. In such a case, one method to improve the “quality” of the model might be to eliminate such an explanatory variable. It should be recognised, though, that such an interference to obtain “meaningful” statistical results would be tantamount to improving the actual measurements. Hence, it was decided to use multiple ridge regression, which employs the lambda (I) parameter in its calculations. By adding the lambda, the value of correlation is reduced to obtain more stable beta coefficients. The lambda (I) parameter is found by trial and error or selected arbitrarily and most often starts with 0.01 increasing by 0.001, until stable estimates can be achieved. In this paper, I = 0.01 was assumed in all calculations. Thus, it is an analytical model where we lose some to gain some. In this case, we gain a calculation model wherein all the explanatory variables are included; yet, in some calculations, the coefficient of determination (R 2) is slightly reduced. The ultimate model demonstrates the actual impact of explanatory variables on the explained variable and the synergies. The summary statistics of the multiple ridge regression coefficient for the entire material and subgroups selected according to SBP and/or DBP are presented in Tables 3, 4, 5, 6, 7, 8, 9 and 10. Calculations of the multiple ridge regression with regard to SBP and DBP were performed separately for the minerals alone and then including two additional variables into the equation: calendar age and BMI. The confidence threshold in the statistical analysis was adopted at p < 0.05. Moreover, ratios of chosen minerals were calculated for the subgroups with normal blood pressure and high blood pressure (SBP and/or DBP). Significant statistical differences of obtained results have been found (Table 11).
For research purposes, an attempt was made at analysing the weekly menu of the canteen at the boarding school, where the studied men were staying. Meals at the school were the sole source of nutrition for the majority of students. Each day, the canteen served three meals. Meat was served once a fortnight. Nutritional analysis was conducted using the Polish software DIETETYK©. It should be taken into account that the analysed foodstuffs may have different nutrient contents, seen as they grew and ripened in a warmer climate than the models introduced to the computer database. It is an attempt to estimate the nutritional content of the food given to all students. The data were collected for 1 week and recalculated (averaged) to daily rations (Table 12).
Result and Discussion
In the questionnaire, none of the students admitted to being an active cigarette smoker. Having said that, only 78 % of subjects provided an answer to the question. More than half of the respondents (53 %) gave a negative answer to the question regarding heart disease, 4 % gave a positive answer, whereas 43 % did not provide an answer at all. Most probably, this is because they had never been comprehensively examined. The blood pressure measurements conducted in the course of the present anthropological study were the first ever for most of them.
Elevated readings in arterial blood pressure SBP ≥ 140 mm Hg were found in 22 % (n = 20) of subjects and the same percentage in the case of DBP ≥ 90 mm Hg. Men whose SBP ≥ 140 mm Hg and/or DBP ≥ 90 mm Hg accounted for the total of 31 % (n = 28) of the studied group. The others, n = 63 (69 %), had normal blood pressure readings (Table 11).
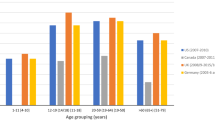
Three men from the analysed group (3.3 %) were in the grade 1 overweight category according to the BMI, 81.3 % (n = 74) of the studied group fell in the normal BMI range, whereas 13.2 % (n = 12) were grade 1 underweight. One man (1.1 %) represented the grade 2 underweight category and another, grade 3 underweight. Analysis of the collected material demonstrates a weak positive correlation of SBP vs. BMI (r = 0.2 for p < 0.05). No correlation was found, though, for DBP and HR vs. BMI. A high positive coefficient of correlation was found in BMI vs. calendar age (r = 0.4 for p < 0.05), which confirms a well-known regularity in biology. Yet, ridge regression analysis shows a weak impact of calendar age and BMI on the variation of blood pressure. In the group with high SBP and/or DBP (n = 28), calendar age and BMI have practically no influence on the coefficient of determination R 2 in accounting for SBP variation, but affect the coefficient of determination R 2 by as little as 2 % in accounting for DBP variation. In the group with SBP ≥ 140 mm Hg (n = 20), calendar age and BMI increase the coefficient of determination R 2 by 8 % in explaining SBP variation and by 5 % in the case of DBP. In the group whose DBP ≥ 90 mm Hg (n = 20), calendar age and BMI have a minimal (2 %) impact on increasing the coefficient of determination R 2 to account for SBP variation. The impact of calendar age and BMI on the increase in the coefficient of determination R 2 in DBP variation (R 2 = 0.3282) is slightly stronger (11 %), though still insignificant from the statistical point of view.
According to the analysis of food offered to the boarders, the daily calorie intake ranged from 1,500 to 2,200 kcal. The Polish National Food and Nutrition Institute recommends that young males eat 3,200–3,700 kcal/day depending on the activity level. The estimates obtained demonstrate that the students received an insufficient amount of calories. In terms of volume, the rations were not small, but with meat often absent from the menu, they would have a short-term satiating effect. This was hardly set off by the fact that in hot climates the need for food is diminished. Students were regularly involved in sports activities. They did not abstain from physical exertion. They participated in team sports such as football and basketball and were happy to spend time in dance classes. On average, proteins accounted for 21.35 % of the energy intake, whereas fats provided 19.3 %, and carbohydrates 59.4 % of the total supplied nutritional energy. Concentrations of analysed minerals in the weekly diet recalculated into daily averages are presented in Table 12.
Among the seven minerals subject to analysis (Table 2), the highest positive correlation of medium intensity vs. DBP r = 0.3 (p < 0.05) was found in Na and K. The correlation of Mg vs. DBP is negative (r = –0.17, p < 0.104). Material analysis also indicates that there is a medium positive correlation of SBP vs. Na (r = 0.3, p < 0.05). The remaining minerals did not present significant associations in correlation analysis, either vs. SBP or vs. DBP.
The role and significance of Na in inducing arterial hypertension is widely recognised [25]. The study conducted by Zoccali et al. [26] demonstrated a linear association between Na consumption and daily blood pressure figures in middle-aged individuals [27, 28]. Yet, the evaluation of impact sodium intake has on the development of hypertension in the general population remains a subject of controversy. The differences of opinion may be related to the concentrations of other minerals in the body, whose interdependencies and interactions have not been sufficiently recognised to date. Research studies [25, 29] show a positive association between average blood pressure and Na concentration, with an accompanying negative correlation with Mg levels. The present results of the correlation analysis confirm the positive correlation of SBP and DBP vs. Na (r = 0.29 and r = 0.25, respectively) and the negative correlation of both SBP and DBP vs. Mg (r = –0.03 and r = –0.17, respectively). Regression analysis does not show a deviation from the above rule. In subjects with high SBP (n = 20), as little as 2 % (R 2 = 0.02) of variation in high SBP is explained by Mg. Very similar values are observed in the development of high DBP. Increased Mg supply affects serum concentration of Mg while at the same time increasing its elimination in urine.
Ascherio et al. [30] determined a reverse correlation between SBP and DBP and consumption of Ca, Mg and K. In people with hypertension, as well as those with normal blood pressure, an increased dietary intake of K has a hypotensive effect [31, 32]. Thus, the Na/K ratio in the body is important. In the study group, the mean Na/K ratio is 1.60(±0.59):1, ranging from 0.74:1 to 3.71:1. The optimal Na/K ratio for the human body is approximately 2:1. Regression analysis shows a moderate impact of K on developing high SBP (n = 20) and high DBP (n = 20). Taking into account that the material analysed for mineral content is hair, it must be recognised that the Na/K ratio findings are relatively favourable for the studied group. The reason for this should be sought in the quality and quantity of nutrients found in natural foodstuffs. They contain more potassium than the contemporary diet, characterised by reversed proportions: high Na and low K concentration [33]. Such a diet can adversely affect the ratio and therefore have a stronger impact on blood pressure. The hypotensive effect of high K intake is neutralised by the accompanying high supply of Na typical of mass catering. Based on the information collected on the food provided at the school in question, kitchen salt was one of the very few condiments used in the canteen. For individuals with SBP ≥ 140 mm Hg (n = 20), the mean Na/K ratio amounts to 1.53(±0.66):1, with range from 0.76:1 to 3.71:1. In the group whose DBP ≥ 90 mm Hg, the mean Na/K ratio amounts to 1.47(±0.45):1, ranging from 0.76:1 to 2.56. In individuals whose SBP ≥ 140 mm Hg and/or DBP ≥ 90 mm Hg, the mean Na/K ratio amounts to 1.54(±0.60):1, ranging from 0.76:1 to 3.76:1.
In the literature, the role of Ca and Mg concentrations in the development of arterial hypertension is emphasised. Opinions regarding the role played by Ca in this respect seem to be divided. Excess dietary Ca, similarly to a deficiency of Mg, is linked with higher incidence of hypertension. On the other hand, a high level of Ca originating from a diet rich in this mineral prevents elevated blood pressure caused by a high sodium intake [34]. Correlation analysis of Ca vs. Zn, Fe, Na and K demonstrates negative correlations (r = –0.09, r = –0.09, r = –0.07 and r = –0.17, respectively). There is no association between Ca vs. Mg, as they are usually antagonistic in the human body and are subject to strong homeostatic control. Notably, however, a high Ca/Mg ratio was found in the researched group, amounting to 173(±60.1):1, ranging from 67:1 to 366:1. In this case, it may prove a strong impact of Ca levels on the concentrations of other trace elements. Calcium remains associated to age (r = 0.29, p < 0.05). The important role played by Ca in the changes of BMI has been recognised [35]. Assessing the direct impact of Ca on blood pressure is adversely affected by the high SD and wide spread of results. The Ca/Mg ratio is similar across the analysed group. In individuals whose SBP ≥ 140 mm Hg (n = 20), the mean Ca/Mg ratio amounts to 177.77(±75.20):1. For those whose DBP ≥ 90 mm Hg (n = 20), the mean Ca/Mg ratio amounts to 188.44(±74.54):1, whereas in individuals whose SBP ≥ 140 mm Hg and/or DBP ≥ 90 mm Hg (n = 28), the mean Ca/Mg ratio amounts to 179.98(±71.55):1.
Iron probably does not feature significantly in the direct development of arterial hypertension. Yet, excess Fe blocks the absorption of other minerals, which may be a key factor in the assessment of impact of hair mineral content on blood pressure [36, 37]. The above principle is confirmed by the results of the regression analysis of the collected material. In the group of men with high SBP (n = 20), in the analysis of impact of minerals on SBP, excluding Fe out of the regression equation led to a drop in the coefficient of determination R 2 from 0.26 down to 0.18. Yet, excluding Fe out of the regression equation does not in any way account for the change of DBP in the same group of individuals with high SBP. In the group of men with high DBP (n = 20), analysis of the regression equation to determine the influence of mineral levels on SBP shows that the degree of determination R 2 declines after excluding Fe from R 2 = 0.68 to R 2 = 0.63. In both equations, the values of Ca and Zn remain statistically significant. The value of R 2 changes minimally in the analysis of regression equation concerning the influence of minerals on DBP in the group with high DBP. In the analysed material, Fe is characterised by a high correlation coefficient vs. K (r = 0.48, p < 0.000).
Research shows that impaired metabolism of zinc and copper may cause hypertension [38, 39]. It has been found that zinc has an antagonistic effect on copper absorption. In the analysis of ridge stepwise regression for the group of men with high DBP (n = 20), the values of Cu, as well as Zn and Fe, were not included in the equation as significant variables accounting for DBP. However, in the group with high SBP and/or DBP, Zn and Cu were included in the regression analysis to account for SBP variation. Many foreign substances in foodstuffs hinder Cu absorbability from food; hence, copper deficiency is relatively common. It is important to look out for a decline of the Zn/Cu ratio. Zinc plays an important role in the activity of zinc-dependent enzymes [33]. It also has antioxidant properties and stabilises cell membranes [40]. On the other hand, Cu is a necessary trace element found in enzymes catalysing oxidoreduction reactions [41]. In the analysed material, Zn displays a positive correlation with a weak or medium intensity vs. Mg, Fe, Cu, K and Na (r = 0.26, r = 0.26, r = 0.22, r = 0.32 and r = 0.22, respectively). The optimal Zn/Cu ratio should range between 8:1 and 15:1 [33]. The mean Zn/Cu ratio in the studied group amounts to 14(±6.88):1, which should be recognised as a very good result. It is, however, worth noting that the spread of Zn/Cu ratios in the studied group is very broad, ranging from 3:1 to 37:1. In individuals whose SBP ≥ 140 mm Hg, the mean Zn/Cu ratio amounts to 15(±6.82):1. In the group with elevated DBP ≥ 90 mm Hg, the mean Zn/Cu ratio is 14(±8.30):1. In men whose SBP ≥ 140 mm Hg and/or DBP ≥ 90 mm Hg, the mean Zn/Cu ratio is 14.07(±8.10):1. This may indicate a high individual variability in absorbing these particular minerals from food.
Analysis of ridge regression findings for the researched group (n = 91) shows that the minerals under scrutiny account for SBP variation in 13 % and in 15 % for DBP variation. After two additional variables—calendar age and BMI—are included in regression analysis, the ultimate coefficient of determination (R 2) changes for SBP and remains the same for DBP (R 2 = 0.194 and R 2 = 0.156, respectively).
In the group whose SBP and/or DBP (n = 28) exceed the adopted thresholds, the multiple ridge regression analysis explains 50 % of SBP levels and 12 % of DBP levels—excluding the variables of BMI and calendar age. After the latter are included, the ultimate coefficient of determination (R 2) changes minimally for SBP, and in the case of DBP, it increases by 2 %.
In the group whose DBP ≥ 90 mm Hg (n = 20), the final result of multiple ridge analysis shows that mineral contents account for 22 % of high DBP readings in this group and 68 % in the case of SBP. Two additional variables, i.e. BMI and calendar age, increase these percentages to 33 % for DBP and 69 % for SBP.
The multiple ridge analysis of hair mineral content in the group with SBP ≥ 140 mm Hg (n = 20) accounts for SBP in 27 % and for DBP in 16 %. After including the variables of BMI and calendar age, the ultimate coefficient of determination (R 2) for SBP goes up to 0.35 and for DBP up to 0.21.
Such high coefficients of determination in assessing the impact of selected minerals, BMI and calendar age on elevated SBP and elevated DBP seem to justify the claim that the adopted model of statistical calculation is appropriate.
Researchers studying changes in arterial blood pressure raise the issue that there are no systematic and exhaustive publications of results of longitudinal studies on the people of Africa [6]. Nevertheless, findings of European and American population studies identify changes in blood pressure caused by industrialisation and migration [42–44]. Migration plays a particularly important role, as it directly affects such factors as diet, salt consumption, stress, method of food preparation, decline in potassium intake, consumption of vegetable and animal proteins and fats [45–47]. Blood pressure is lower in those population groups where lifestyles do not change due to migration [48]. In the analysed group, blood pressure readings may have been slightly affected by staying at the boarding school. In the course of the study, the students were also asked about the location of their parental residence (urban vs. rural). Of the respondents, 40 % answered that their mother lived in a rural area, and 60 % decided that their father lived in a town/city on a permanent basis. Yet, a vast majority of the respondents (86 %) identified themselves as rural inhabitants. This may be a sign of the parental model, as well as an indication that, in many cases, the respondents remained in the care of relatives living in the countryside. Migrations also have an impact on the changes in blood pressure of Africans inhabiting their native environments [49–51]. Research findings of other authors concerning blood pressure in Bantu populations in native environments diverge from the present study conducted on what is practically the same age group [43, 44, 52, 53]. This may indicate progressive environmental and dietary changes, which affect the present results, as well as a general upward trend in blood pressure in Africa. One important common element uncovered by these different studies is low awareness of the threats related to high or low blood pressure. None of the students from the group with abnormal blood pressure was aware of his condition or remained under regular medical supervision.
Comparing these findings regarding the impact of hair mineral content on blood pressure is difficult. In the available literature on Bantu or any other black populations inhabiting native environments, the authors usually base mineral analysis on the biochemical analysis of blood or urine [51, 52, 54]. The ever-present civilisational stress more and more often affects the indigenous communities, too, and impacts Africans’ health. Research studies show that the incidence of diseases related to hypertension is on the rise [55–57]. It is a worldwide tendency and also affects the African continent.
Conclusions
Hair analysis used to determine mineral content in the body may be an auxiliary tool in identifying the links between factors leading to the development of hypertension. Moreover, the hair as a material for analysis of the content of trace elements in organism can be helpful in evaluation of the health status of examined populations living in hardly accessible environments.
References
Blankson JM, Larbi EB, Pobee JOM, Pole DJ, Ikeme AC (1977) Blood pressure levels of African children. J Chronic Dis 30:735–743
Reeves RD, Jolley KW, Buckley PD (1975) Lead in human hair: relation to age, sex and environmental factors. Bull Environ Contam Toxicol 14:579–587
Oviasu VO, Okupa FE (1980) Relation between hypertension and occupational factors in rural and urban Africans. Bull World Health Organ 58(3):485–489
Daniels SR, Heiss G, Davis CE, Hames CG, Tyroler HA (1988) Race and sex differences in the correlates of blood pressure change. Hypertension 11(3):249–255
Perrone L, Moro R, Caroli M, Di Toro R, Gialanella G (1996) Trace elements in hair of healthy children sampled by age and sex. Biol Trace Elem Res 51(1):71–76
Lawes CMM, Hoorn SV, Law MR, Elliott P, MacMahon S, Rodges A (2004) High blood pressure. In: Ezzati M, Lopez AD, Rodgers A, Murray CJL (eds) Comparative quantification of health risks. Global and regional burden of disease attributable to selected major risk factors, vol 1. WHO, Geneva
Prasad A (1977) Trace elements in human health and disease. Academic, New York
Prasad AS (1985) Essential trace elements in human health and disease. J Am Coll Nutr 4(1):1–2
Fraga CG, Oteiza PI, Keen CL (2005) Trace elements and human health. Mol Aspects Med 26(4–5):233–234
Bhandari B (1983) Trace elements in human health and disease. Q Med Rev 34(4):1–33
Kaufman JS, Owoaje EE, Rotimi CN, Cooper RS (1999) Blood pressure change in Africa: case study from Nigeria. Hum Biol 71(4):641–657
Taylor A (1986) Usefulness of measurements of trace elements in hair. Ann Clin Biochem 23:364–378
Gibson RS, Anderson BM, Scythes CA (1983) Regional differences in hair zinc concentration: a possible effect of water hardness. Am J Clin Nutr 37:37–42
Bass DA, Hickok D, Quig D, Urek K (2001) Trace elements analysis in hair: factors determining accuracy, precision, and reliability. Altern Med Rev 6(5):472–481
Iyengar V, Woittiez J (1988) Trace elements in human clinical specimens: evaluation of literature data to identify reference values. Clin Chem 34:474–481
Passwater R, Cranton EEM (1983) Trace elements, hair analysis and nutrition. Keats, New Canaan
Swaminathan R (2003) Magnesium metabolism and its disorders. Clin Biochem Rev 24(2):47–66
Dimitrova AA, Strashimirov D, Betova T, Russeva A, Alexandrova M (2008) Zinc content in the diet affects the activity of Cu/ZnSOD, lipid peroxidation and lipid profile of spontaneously hypertensive rats. Acta Biol Hung 59(3):305–314
Windisch W (2002) Interaction of chemical species with biological regulation of the metabolism of essential trace elements. Anal Bioanal Chem 372:421–425
Yogi A, Callera GE, Antunes TT, Tostes RC, Touyz RM (2010) Vascular biology of magnesium and its transporters in hypertension. Magnes Res 23(4):S207–S215
Guidelines Subcommittee (1999) World Health Organization—International Society of Hypertension guidelines for the management of hypertension. J Hypertens 17:151–183
Martin R, Saller K (1958) Lehrbuch der anthropologie in systematischer darstellung. Gustav Fischer Verlag Stuttgart, Stuttgart
WHO EXPERT COMMITTEE (1995) Recommended measurement protocols and derivation of indices. In: Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. WHO Technical Report Series, Geneva, pp 450–452
Rębacz E, Baranowska-Bosiacka I, Chlubek D (2010) The content of selected chemical elements in the hair of young men of the Bantu language group from Tanzania versus environmental and social conditioning. Biol Trace Elem Res 137:262–279
Gruchow HW, Sobocinski KA, Barboriak JJ (1988) Calcium intake and the relationship of dietary sodium and potassium to blood pressure. Am J Clin Nutr 48:1463–1470
Zoccali C, Mallamaci F, Leonardis D (1994) Assessment of the salt–arterial pressure relationship in mild hypertensive subjects by 24-hour ambulatory monitoring. Clin Sci 87:635–639
Hedayati SS, Minhajuddin AT, Ijaz A, Moe OW, Elsayed EF, Reilly RF, Huang CL (2012) Association of urinary sodium/potassium ratio with blood pressure: sex and racial differences. Clin J Am Soc Nephrol 7(2):315–322
Gariballa SE (2000) Nutritional factors in stroke. Br J Nutr 84(1):5–17
Touyz RM, Milne FJ (1995) Alterations in intracellular cations and cell membrane ATP-ase activity in patients with malignant hypertension. J Hypertens 13:867–874
Aschiero A, Hennekens C, Willett WC, Sacks F, Rosner B, Manson J, Witteman J, Stampfer MJ (1996) Prospective study of nutritional factors, blood pressure, and hypertension among US women. Hypertension 27:1065–1072
He FJ, Mac Gregor GA (1999) Potassium intake and blood pressure. Am J Hypertens 12:849–851
Wu G, Tian H, Han K, Xi Y, Yao Y, Ma A (2006) Potassium magnesium supplementation for four weeks improves small distal artery compliance and reduces blood pressure in patients with essential hypertension. Clin Exp Hypertens 28(5):489–497
The Nutrition Digest of Essential Nutrients (2005) Enerex Botanicals Ltd., Canada. http://www.enerex.ca/articles/nutrition_digest.pdf. Cited 6 February 2012
Ono A, Ando K, Fujita T (1994) High calcium diet prevents salt-induced hypertension and impairment of renal hemodynamics in young spontaneously hypertensive rats. J Cardiovasc Pharmacol 23:624–628
Zemel MB (2001) Calcium modulation of hypertension and obesity: mechanisms and implications. J Am Coll Nutr 20(suppl5):428S–435S
Lieu PT, Heiskala M, Peterson PA, Yang Y (2001) The roles of iron in health and disease. Mol Aspects Med 22:1–87
Duffy SJ, Biegelsen ES, Holbrook M, Russell JD, Gokce N, Keaney JF, Vita JA (2001) Iron chelation improves endothelial function in patients with coronary artery diesease. Circulation 103:2799–2804
Saltman P (1983) Trace elements and blood pressure. Ann Intern Med 98:823–827
Tubek S (2001) Increased absorption of zinc from alimentary tract in primary arterial hypertension. Biol Trace Elem Res 83(1):31–38
McClain C, Morris P, Hennig B (1995) Zinc and endothelial function. Nutrition 11:117–120
Linder MC, Hazegh-Azam M (1996) Copper biochemistry and molecular biology. Am J Clin Nutr 63:797S–811S
Poulter N, Khaw KT, Hopwood BE, Mugambi M, Peart WS, Rose G, Sever PS (1984) Blood pressure and associated factors in rural Kenyan community. Hypertension 6:810–813
Swai AB, McLarty DG, Kitange HM, Kilima PM, Tatalla S, Keen N, Chuwa LM, Alberti KG (1993) Low prevalence of risk factors for coronary heart disease in rural Tanzania. Int J Epidemiol 22(4):651–659
Edwards R, Unwin N, Mugusi F, Whiting D, Rashid S, Kissima J, Aspray TJ, Alberti KG (2000) Hypertension prevalence and care in an urban and rural area of Tanzania. J Hypertens 18(2):145–152
Baumslag N, Petering HG (1976) Trace metal studies in Bushman hair. Arch Environ Health 31(5):254–257
He J, Klag MJ, Whelton PK, Chen JY, Mo JP, Qian MC, Mo PS, He GQ (1991) Migration, blood pressure pattern, and hypertension: the Yi migrant study. Am J Epidemiol 134(10):1085–1101
Njelekela M, Sato T, Nara Y, Miki T, Kuga S, Noguchi T, Kanda T, Yamori M, Ntogwisangu J, Masesa Z, Marshalla Y, Mtabaji J, Yamori Y (2003) Nutritional variation and cardiovascular risk factors in Tanzania—rural–urban difference. S Afr Med J 93(4):295–299
Poulter NR, Khaw KT, Sever PS (1988) Higher blood pressures of urban migrants from an African low-blood pressure population are not due to selective migration. Am J Hypertens 1:143S–145S
Pobee JO, Larbi EB, Belcher DW, Wurapa FK, Dodu SR (1977) Blood pressure distribution in a rural Ghanian population. Trans R Soc Trop Med Hyg 71(1):66–72
Seedat YK, Seedat MA, Hackland DBT (1982) Biosocial factors and hypertension in the urban and rural Zulus. S Afr Med J 61:999–1002
Poulter N, Khaw KT, Hopwood BEC, Mugambi M, Peart WS, Rose G, Sever PS (1984) Blood pressure and its correlates in an African tribe in urban and rural environments. J Epidemiol Community Health 38(3):181–185
Kesteloot H, Ndam N, Sasaki S, Kowo M, Seghers V (1996) A survey of blood pressure distribution in Pygmy and Bantu population in Cameroon. Hypertension 27:108–113
Bovet P, Ross AG, Gervasoni JP, Mkamba M, Mtasiwa DM, Lengeler C, Whiting D, Paccaud F (2002) Distribution of blood pressure, body mass index and smoking habits in the urban population of Dar es Salaam, Tanzania, and association with socioeconomic status. Int J Epidemiol 31:240–247
M’Buyamba-Kabangu JR, Fagard R, Lijnen P, Mbuy wa Mbuy R, Staessen J, Amery A (1986) Blood pressure and urinary cations in urban Bantu of Zaire. Am J Epidemiol 124(6):957–968
Chiolero A, Gervasoni JP, Rwebogora A, Balampana M, Paccaud F, Bovet P (2006) Difference in blood pressure readings with mercury and automated devices: impact on hypertension prevalence estimates in Dar es Salaam, Tanzania. Eur J Epidemiol 21:427–433
Cappuccio FP, Micah FB, Emmett L, Kerry SM, Antwi S, Martin-Peprah R, Philips RO, Plange-Rhule J, Eastwood JB (2004) Prevalence, detection, management, and control of hypertension in Ashanti, West Africa. Hypertension 43:1017–1022
Mufunda J, Scott LJ, Chifamba J, Matenga J, Sparks B, Cooper R, Sparks H (2000) Correlates of blood pressure in an urban Zimbabwean population and comparison to other populations of African origin. J Hum Hypertens 14(1):65–73
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Rębacz-Maron, E., Baranowska-Bosiacka, I., Gutowska, I. et al. Blood Pressure and Levels of Fe, Ca, Mg, Zn, Cu, Na and K in the Hair of Young Bantu Men from Tanzania. Biol Trace Elem Res 151, 350–359 (2013). https://doi.org/10.1007/s12011-012-9578-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-012-9578-3