
Abstract
Background
Little information exists concerning the variability of presentation and differences in treatment methods for developmental dysplasia of the hip (DDH) in children < 18 months. The inherent advantages of prospective multicenter studies are well documented, but data from different centers may differ in terms of important variables such as patient demographics, diagnoses, and treatment or management decisions. The purpose of this study was to determine whether there is a difference in baseline data among the nine centers in five countries affiliated with the International Hip Dysplasia Institute to establish the need to consider the center as a key variable in multicenter studies.
Questions/purposes
(1) How do patient demographics differ across participating centers at presentation? (2) How do patient diagnoses (severity and laterality) differ across centers? (3) How do initial treatment approaches differ across participating centers?
Methods
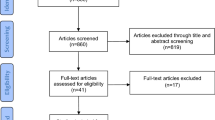
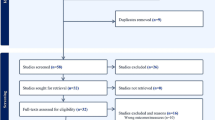
A multicenter prospective hip dysplasia study database was analyzed from 2010 to April 2015. Patients younger than 6 months of age at diagnosis were included if at least one hip was completely dislocated, whereas patients between 6 and 18 months of age at diagnosis were included with any form of DDH. Participating centers (academic, urban, tertiary care hospitals) span five countries across three continents. Baseline data (patient demographics, diagnosis, swaddling history, baseline International Hip Dysplasia Institute classification, and initial treatment) were compared among all nine centers. A total of 496 patients were enrolled with site enrolment ranging from 10 to 117. The proportion of eligible patients who were enrolled and followed at the nine participating centers was 98%. Patient enrollment rates were similar across all sites, and data collection/completeness for relevant variables at initial presentation was comparable.
Results
In total, 83% of all patients were female (410 of 496), and the median age at presentation was 2.2 months (range, 0–18 months). Breech presentation occurred more often in younger (< 6 months) than in older (6–18 months at diagnosis) patients (30% [96 of 318] versus 9% [15 of 161]; odds ratio [OR], 4.2; 95% confidence interval [CI], 2.3–7.5; p < 0.001). The Australia site was underrepresented in breech presentation in comparison to the other centers (8% [five of 66] versus 23% [111 of 479]; OR, 0.3, 95% CI, 0.1–0.7; p = 0.034). The largest diagnostic category was < 6 months, dislocated reducible (51% [253 of 496 patients]); however, the Australia and Boston sites had more irreducible dislocations compared with the other sites (ORs, 2.1 and 1.9; 95% CIs, 1.2–3.6 and 1.1–3.4; p = 0.02 and 0.015, respectively). Bilaterality was seen less often in older compared with younger patients (8% [seven of 93] versus 26% [85 of 328]; p < 0.001). The most common diagnostic group was Grade 3 (by International Hip Dysplasia Institute classification), which included 58% (51 of 88) of all classified dislocated hips. Splintage was the primary initial treatment of choice at 80% (395 of 496), but was far more likely in younger compared with older patients (94% [309 of 328] versus 18% [17 of 93]; p < 0.001).
Conclusions
With the lack of strong prognostic indicators for DDH identified to date, the center is an important variable to include as a potential predictor of treatment success or failure.
Similar content being viewed by others

Introduction
Developmental dysplasia of the hip (DDH) is a spectrum of hip abnormalities that range from mild dysplasia in a reduced hip to severe dysplasia in a frankly dislocated hip [4]. DDH is the most common hip disorder in the pediatric population, with 1% to 3% of all newborns being diagnosed at birth [13, 26]. However, the true incidence of DDH is difficult to quantify as a result of important variations in diagnostic criteria and ethnic and cultural differences [22, 23]. The standard diagnosis procedure remains clinical examination of all newborns; however, not all patients can be diagnosed by this method. A delay in detection can lead to the need for more complex treatments later in life; consequently, the importance of diagnosing and treating DDH in early infancy is recognized globally.
Once diagnosed, there is also much controversy surrounding treatment approaches. Splintage is typically an effective treatment for infants with DDH, but there are variations in splint/brace type, indications for treatment, and duration of treatment as well as complications associated with different brace types [26]. In fact, the recent release of new DDH clinical practice guidelines highlighted the lack of evidence to support or refute a given diagnostic or treatment approach [1]; consequently, there is no standardized practice for DDH diagnosis and management.
Multicenter studies can be a valuable tool to capture the breadth of presentations of a given condition or disease. The inherent advantages of prospective, multicenter studies are well documented; however, data from different centers can differ in terms of important variables such as patient demographics, diagnoses, and treatment or management decisions, potentially introducing bias or compromising the validity of the results. This is commonly dealt with by controlling for center-specific confounders such that the effect does not impact the overall analysis. However, this variability across centers can also be vitally important to provide a complete picture of the scope of diagnoses, risk factors, and treatment options present for a particular condition or disease, and the study center may indeed represent a key predictive variable for treatment outcomes. Instead of controlling for center variability by eliminating its effects, we argue that instead, the center should be considered as a predictive variable in regression analysis of outcomes.
The International Hip Dysplasia Institute (IHDI) began a prospective, multicenter, observational cohort study of children younger than 18 months old with DDH. This study aims to assess center variation at patient presentation to establish a baseline from which future comparative treatment and outcome studies can be developed and to demonstrate the need to include the center as a predictive variable.
We therefore asked: (1) How do patient demographics differ across participating centers at presentation? (2) How do patient diagnoses (severity and laterality) differ across centers? (3) How do initial treatment approaches differ across participating centers?
Patients and Methods
Study Design
Data provided by a multicenter prospective hip dysplasia study database were analyzed from 2010 to April 2015. Study data were collected and managed using REDCap electronic data capture tools (Vanderbilt University, Nashville, TN, USA). Baseline data, including patient demographics, diagnosis (dislocated or dysplastic, dislocation type), radiographic IHDI classification [16], and initial treatment, were compared across all nine centers. These nine participating centers represent five different countries on three different continents. All centers are tertiary care hospitals located in major cities.
Inclusion and Exclusion Criteria
Children younger than 6 months of age at baseline were included in the analysis if they had at least one frankly dislocated hip, whereas children between 6 and 18 months of age at baseline were included if they had at least one hip with some form of dysplasia. Only initial presentations of DDH were included, and all diagnoses were required to be confirmed by ultrasonographic or radiographic imaging before brace or surgical treatment. Joint laxity (reducible or irreducible) was required to be reported for dislocated hips to assign patients to one of the five major diagnostic categories: < 6 months of age at diagnosis with dislocated reducible hip(s), < 6 months of age with dislocated irreducible hip(s), 6 to 18 months of age with dislocated reducible hip(s), 6 to 18 months of age with dislocated irreducible hip(s), and 6 to 18 months of age with dysplastic hip(s). Most centers focused on the recruitment of patients in diagnosis categories one to four; thus, the distribution of patients in group five is widely variable across centers and is treated separately here.
Patients with known or suspected neuromuscular, collagen, chromosomal, or lower extremity congenital anomalies or patients < 6 months of age at baseline who did not have a frankly dislocated hip (that is, a subluxated or dysplastic hip) were excluded from the study. Clinical diagnoses of dislocation or dysplasia without radiographic confirmation and patients who had previously received treatment with orthosis or surgery were also excluded.
Study Population
In total, 496 patients were included in analysis with site enrollment ranging from 10 (the Philadelphia site) to 117 (the UK site). Of these patients, 66% (328 of 496) were < 6 months old at baseline (younger group, median age 1 month [0–6 months]), and 34% (168 of 496) were 6 to 18 months old (older group, median age 9 months [6–18 months]); 83% (410 of 496) of all patients were female. Ultrasound imaging confirmed diagnosis in 317 of 496 patients (313 in the younger group, four in the older group), whereas radiography confirmed diagnosis in 179 patients (15 in the younger group, 164 in the older group).
Variables, Outcomes, and Measures Assessed
Variables studied included basic patient demographics such as age at presentation, sex and fetal presentation, diagnosis (dislocated and reducible or irreducible or dysplastic/dislocatable), laterality, history of swaddling, dislocation severity by radiographic analysis, and initial treatment. Initial diagnosis was made by clinical assessment followed by ultrasound or radiographic imaging analysis. Less than 35% coverage of the femoral head on ultrasound was considered a dislocation. Severity of dislocation on radiography was assessed using the IHDI classification system [16]. The IHDI classification system uses the midpoint of the proximal femoral metaphysis as a reference landmark to describe the femoral head position in relation to the acetabulum. An IHDI Grade 1 represents a reduced hip, Grade 2 represents a subluxed and/or dysplastic hip, whereas Grades 3 and 4 represent dislocated hips. This classification system has been found to have excellent interrater reliability with intraclass correlation coefficients of 0.90 and 0.95 for right and left hips, respectively [16].
On diagnosis, patients were treated in accordance with the individual surgeon/center standard of care and decision-making process. Treatments included observation, orthosis application, and serial monitoring or surgery (closed or open reduction).
Data Completeness
For included, eligible patients, there was a high level of data completeness across all centers for each analyzed endpoint. Of the 496 included patients, there was 100% reporting of age, sex, dislocation type, and initial treatment approach. There was 97% reporting of fetal presentation (479 of 496) and 96% reporting of family history (477 of 496). With recruitment rates ranging from 95% to 100% across all centers and high rates of data completion for the evaluated endpoints, center-to-center differences should not be impacted by patient capture or completion bias.
Statistical Analysis
Basic descriptive statistics were performed on all baseline data. Chi-square tests were performed to determine differences between centers for important demographic, diagnostic, and treatment variables. All statistics were calculated with a minimum statistical significance of p < 0.05.
Results
Patient Demographics
Single-center female-to-male patient ratios were consistent with the total study population, comprised of 83% female patients (410 of 496) and 17% male patients (86 of 496; Table 1). Breech presentation occurred more often in younger (< 6 months) patients than in older (6-18 months) patients (30% [96 of 318] versus 9% [15 of 161]; odds ratio [OR], 4.2; 95% confidence interval [CI], 2.3–7.5; p < 0.001). Breech presentation was less likely at the Australia site in comparison to the other centers (8% [five of 66] versus 23% [111 of 479]; OR, 0.3; 95% CI, 0.1–0.7; p = 0.034) (Table 1). A reported family history of DDH was less common at the Mexico and Orlando sites in comparison to the total study population (13% [five of 39] and 4% [one of 24] versus 31% [148 of 477]; ORs, 0.3 and 0.1; p = 0.0162 and p = 0.005, respectively). In contrast, a reported family history was more common at the UK site (44% [51 of 115] versus 31% [148 of 477]; OR, 1.8; 95% CI, 1.2–2.7; p = 0.009) (Table 1).
Diagnosis (severity and laterality)
Patient numbers ranged from 34 (7% of total enrolled) in the 6- to 18-month dislocated reducible to 253 (53% of total enrolled) in the < 6-month dislocated reducible group. Additionally, 14 patients had one reducible and one irreducible dislocated hip (Table 2).
In the younger group, 77% (253 of 328) of patients had a unilateral or bilateral reducible dislocation, whereas 19% (62 of 328) had a unilateral or bilateral irreducible dislocation and 4% (13 of 328) had bilateral dislocations, one reducible and one irreducible. In older patients, diagnoses were varied across centers (p < 0.001). In total, 20% (34 of 168) were dislocated reducible, 35% (58 of 168) dislocated irreducible, and 45% (75 of 168) dysplastic. However, the majority of dysplastic patients were contributed by one center; thus, that group is consequently considered separately than the 6- to 18-month dislocated patients. Overall, the Australia and Boston sites had more irreducible hips in comparison to the other sites (47% [30 of 64] and 44% [20 of 45] versus 29% [120 of 496]; ORs, 2.1 and 1.9; 95% CIs, 1.2–3.6 and 1.1–3.4; p = 0.02 and 0.015, respectively). Across all centers and both age groups, the left hip was more commonly dislocated with 223 of 496 patients classified with a unilateral left dislocation (53%; Table 2). Unilateral right dislocations and bilateral cases were comparable in number with 106 and 92 patients, respectively (Table 2). However, older patients were less likely than younger patients to present with a bilateral dislocation (8% [seven of 93] versus 26% [85 of 328]; OR, 0.2; 95% CI, 0.1–0.5; p < 0.001). Dislocated hip laterality was relatively consistent across centers with the exception of the Orlando and Australia sites. These centers had more and fewer patients with bilateral DDH, respectively (22% [11 of 25] and 6% [four of 62]; ORs, 2.8 and 0.2; 95% CIs, 1.2–6.4 and 0.1–0.7; p < 0.001). There were 75 patients enrolled in the 6- to 18-month dysplastic category (no dislocation). Of these patients, 9% (seven of 75) were unilateral left, 5% (four of 75) were unilateral right, and 85% (64 of 75) were bilateral.
The IHDI classification was used to determine the severity of the dislocation in patients diagnosed by radiograph. In total, 35 right and 53 left dislocated hips were graded on enrollment into the study. Across all centers, Grade 3 was the most common classification, accounting for 58% (51 of 88) of all graded dislocated hips. This observation was consistent at individual centers except San Diego and Vancouver having equal numbers of Grade 3 and 4 hips.
Initial Treatment
Splintage was the most common initial treatment of choice across all centers with 80% (395 of 496) of patients having an orthosis applied at the baseline visit. Preoperative observation was the second most common initial treatment (15% [73 of 496]) followed by surgery at baseline (6% [28 of 496]). Initial treatment choices varied widely among centers, and there were also marked differences in treatment trends between the younger and older groups (Table 3). In patients with a dislocation, the younger group was more likely than the older group to have an orthosis applied as the initial treatment approach (94% [309 of 328] versus 18% [17 of 93]; OR, 72.7; 95% CI, 36–147; p < 0.001). In contrast, the older group was more likely to directly receive surgery than the younger group (24% [22 of 93] versus 2% [six of 328]; OR, 16.6; 95% CI, 6.5–42.5; p < 0.001). Similar to the younger group, 92% (69 of 75) of patients in the 6- to 18-month dysplastic group were treated by orthoses.
The predominant orthosis was the Pavlik harness, used for 324 patients (87% of those initially treated with an orthosis, 69% overall). The Australia site was the only exception to this trend using the Denis Browne splint on 88% (21 of 24) of its orthosis cases. The use of alternative orthoses demonstrated center-specific preferences. The Australia site contributed all instances of Denis Browne use in patients, the San Diego site contributed 19 of 23 instances of Rhino Cruiser (Rhino Pediatric Orthopaedic Designs, Inc, San Diego, CA, USA) use, the Orlando site contributed all instances of Plastizote use, and the Toronto site contributed all instances of Van Rosen use.
Discussion
There is general agreement that pediatric orthopaedics needs more prospective study groups and clinical trials [11, 19]. The Harms Study Group (HSG), Research on Osteochondritis Dessicans of the Knee (ROCK), and International Perthes Study Group (IPSG) present valuable examples within the pediatric orthopaedic field of the power of study groups to produce prospective data [18]. Multicenter studies often control for center-to-center differences by treating these differences as confounding variables. It is not common, however, for large, prospective studies to include the center as a variable in multivariate/regression analyses; for example, the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST) [28], among others [5, 21, 25, 30]. In DDH specifically, the recent American Academy of Orthopaedic Surgeons clinical practice guidelines highlighted the lack of evidence to support specific diagnostic or treatment approaches in DDH, which has resulted in wide variation in clinical care both within and between centers [1]. To our knowledge, this international, multicenter prospective observational study is the first of its scope established with the goal of assessing various forms of treatment and outcomes in DDH. We found there is substantial variability across centers in terms of patient demographics, including fetal presentation and family history, as well as patient diagnoses, including both severity of the condition and laterality. Additionally, there were marked differences across centers in terms of the initial treatment approach.
There are several limitations to this study. First, the physical examination for DDH diagnosis can be subjective and prone to interpretation by the individual observer. A requirement for either ultrasound or radiographic confirmation of diagnosis in this study helps to reduce this subjectivity; however, ultrasound can also be subjective. Second, although the recruitment rate is approximately 90% to 95% across all centers, there are no data for patients who were not recruited into the study. However, the high recruitment rate should negate any substantial effect on population demographics present in the study. Third, not all data fields established at the study outset have complete information, therefore precluding these fields from analysis. For example, there was poor reporting of developmental milestones, height, and weight but relatively good reporting of family history and fetal presentation. Variables with poor reporting or discrepant data were not used in our analysis, eliminating the impact of this missing data. Fourth, ultrasound remains a largely subjective diagnostic procedure for hip dislocations [2]. However, some of that subjectivity was countered by the use of percent coverage of the femoral head as a guide for diagnosis. Finally, environment is a confounding factor. Hip dysplasia at the Mexico site may not necessarily have the same pathology as hip dysplasia at the UK site for example, making it an important variable to consider in multicenter studies.
We found differences between centers in key patient demographics such as age, fetal presentation, and a reported family history of DDH. This demonstrates the importance of having multiple contributing sites to capture a diverse range of patients. With specific sites such as the Australia and Boston centers tending to have an older patient population, patients 6 to 18 months old at diagnosis comprise 34% (168 of 496) of patients in this study. This is a much higher proportion of late-presenting patients than most studies [3, 17, 24]. These differences most likely arose as a result of individual center referral patterns with the nature of each center’s geography to birthing hospitals potentially influencing the patient demographics. Regardless, these differences will allow for a more comprehensive comparison of younger and older patients with DDH than is currently available. Breech presentation at birth, a positive family history, and a history of clinical instability all have been described as risk factors warranting selective screening [1, 4, 6, 20, 27]. However, the extent of association of these risk factors is not well understood or well characterized. We have observed that breech presentation is more likely in the younger patients, which is consistent with previous findings [24]. Consequently, the differences between centers in terms of both fetal presentation and family history may prove valuable in further characterizing these risk factors.
The distribution of diagnoses across centers was relatively consistent in the younger group and distinctly different from the older group. Patients in the younger group most likely presented with a reducible dislocation, whereas patients in the older group most likely presented with an irreducible dislocation. This increased diagnosis of irreducible dislocations in older patients has not previously been reported to our knowledge, because most studies comparing early- versus late-presenting DDH do not report on the reducibility of the dislocation [3, 17, 24]. Consistent with this finding, however, was that the two centers with predominantly older patients, the Australia and Boston sites, both also had substantially more patients diagnosed with an irreducible dislocation than other centers. This may indicate that these sites receive more referrals of severe cases than other sites in the study. Consequently, the treatment algorithm from screening through diagnosis and management may be distinct from other centers and provide an opportunity to compare whole treatment processes as opposed to individual factors. There are few large, multicenter trials that have prospectively collected data on patients with DDH [8, 10, 12]. When we examined laterality, the left hip was more commonly affected, consistent with the literature in the field. However, in contrast with existing literature, we saw more unilateral right than bilateral cases [9], and this observation was surprisingly even more apparent, specifically in the older group. This contrasts with a study by Haasbeek et al. [14], who found that bilaterality was more common in older patients. Taken together, the variability in patient populations across centers in this study provides a comprehensive perspective of the total spectrum of DDH that has not previously been achieved.
Finally, the initial treatment method revealed apparent center-dependent tendencies for splint use and a substantial difference between the younger and older groups regarding surgical management. Consistent with existing literature, the Pavlik harness was overwhelmingly the favored orthosis across all nonoperative patients [7]; however, each center had a distinct second choice of orthosis. Some studies of limited strength have attempted to examine the efficacy of rigid and soft splint use; however, the results are contradictory and the effect sizes small [15, 29]. This natural variation in practice patterns across contributing study centers may allow for a more rigorous comparison of different treatments for patients with similar diagnoses.
This study demonstrated that there were variations of presentation and treatment across centers, which provided the necessary diversity to capture the complex spectrum of DDH. There were contrasts in key areas involving known or suspected risk factors such as fetal presentation and family history, which may indicate or impact screening and diagnosis processes at contributing clinics. For DDH in particular, tremendous variability exists spanning screening and diagnostic practices through treatment management decisions and outcomes. Previous attempts to identify robust or dominant risk factors, screening techniques, and treatment choices have yielded little strong evidence to either support or refute the association of a risk factor or the efficacy of a given clinical decision [1]. Given this lack of evidence, the single strongest predictor of treatment success or failure may be when considering the center as a variable in regression/multivariate analysis. Rather than controlling for center effects as confounders, we may be able to use successful outcomes at a specific center to identify a sequence of factors that contribute to this outcome with more robustness than when considered separately. This study demonstrates that even given large numbers of cases, a single center may not be able to capture the diversity of the DDH spectrum and accompanying treatment choices. Consequently, future studies should consider the center as an important predictor variable in the identification of best practices to institute a standardized diagnostic and management procedure for DDH.
References
American Academy of Orthopaedic Surgeons. Detection and nonoperative management of pediatric developmental dysplasia of the hip in infants up to six months of age. Available at: http://www.aaos.org/research/guidelines/DDHGuidelineFINAL.pdf; 2014. Accessed March 30, 2015.
Aronsson DD, Goldberg MJ, Kling TF, Roy DR. Developmental dysplasia of the hip. Pediatrics. 1994;94:201–208.
Azzopardi T, Van Essen P, Cundy PJ, Tucker G, Chan A. Late diagnosis of developmental dysplasia of the hip: an analysis of risk factors. J Pediatr Orthop B. 2011;20:1–7.
Bialik V, Bialik GM, Blazer S, Sujov P, Wiener F, Berant M. Developmental dysplasia of the hip: a new approach to incidence. Pediatrics. 1999;103:93–99.
Burns PB, Kim HM, Gaston RG, Haase SC, Hammert WC, Lawton JN, Merrell GA, Nassab PF, Yang LJ, Chung KC. Predictors of functional outcomes after simple decompression for ulnar neuropathy at the elbow: a multicenter study by the SUN study group. Arch Phys Med Rehabil. 2014;95:680–685.
Carter CO, Wilkinson JA. Genetic and environmental factors in the etiology of congenital dislocation of the hip. Clin Orthop Relat Res. 1964;33:119–128.
Cashman JP, Round J, Taylor G, Clarke NMP. The natural history of developmental dysplasia of the hip (DDH) after early supervised treatment in the Pavlik harness: a prospective longitudinal follow-up. J Bone Joint Surg Br. 2002;84:418–425.
Dezateux C, Rosendahl K. Developmental dysplasia of the hip. Lancet. 2007;369:1541–1552.
Dunn PM. The anatomy and pathology of congenital dislocation of the hip. Clin Orthop Relat Res. 1976;119:23–27.
Elbourne D, Dezateux C, Arthur R, Clarke NM, Gray A, King A, Quinn A. Ultrasonography in the diagnosis and management of developmental hip dysplasia (UK Hip Trial): Clinical and economic results of a multicentre randomized controlled trial. Lancet. 2002;360:2009–2017.
Engesaeter LB, Furnes O, Havelin LI. Developmental dysplasia of the hip–good results of later total hip arthroplasty: 7135 primary total hip arthroplasties after developmental dysplasia of the hip compared with 59,774 total hip arthroplasties in idiopathic coxarthrosis followed for 0 to 15 years in the Norwegian Arthroplasty Register. J Arthroplasty. 2008;23:235–240.
Finne PH, Dalen I, Ikonomou N, Ulimoen G, Hansen TW. Diagnosis of congenital hip dysplasia in the newborn. Acta Orthop. 2008;79:313–320.
Godward S, Dezateux C. Surgery for congenital dislocation of the hip in the UK as a measure of outcome screening. MRC Working Party on Congenital Dislocation of the Hip. Medical Research Council. Lancet. 1998;351:1149–1152.
Haasbeek JF, Wright JG, Hedden DM. Is there a difference between the epidemiologic characteristics of hip dislocation diagnosed early and late? Can J Surg. 1995;38:437–438.
Heikkila E. Comparison of the Frejka pillow and the von Rosen splint in treatment of congenital dislocation of the hip. J Pediatr Orthop. 1988;8:20–21.
Kelley SP, Cashin MS, Douziech JR, Varghese RA, Mulpuri K. Levels of evidence at the Pediatric Orthopaedic Society of North America Annual Meetings. J Pediatr Orthop. 2010;30:612–616.
Laborie LB, Markestad TJ, Davidsen H, Bruras KR, Aukland SM, Bjorlykke JA, Reigstad H, Indrekvam K, Lehmann TG, Engesaeter IO, Engesaeter LB, Rosendahl K. Selective ultrasound screening for developmental hip dysplasia: effect on management and late detected cases. A prospective survey during 1991-2006. Pediatr Radiol. 2014;44:410–424.
Mulpuri K, Brighton BK. Evidence-based medicine and clinical trials in pediatric orthopaedics. J Pediatr Orthop. 2014;34:S71–S73.
Narayanan U, Mulpuri K, Sankar WN, Clarke NMP, Hosalkar H, Price CT; IHDI Study Group. Reliability of a new radiographic classification for developmental dysplasia of the hip. J Pediatr Orthop. 2015;35:478–484.
Noordin S, Masood U, Hafeez K, Nawaz H. Developmental dysplasia of the hip. Orthop Rev. 2010;2:73–78.
Rampersaud YR, Fisher C, Yee A, Dvorak MF, Finkelstein J, Wai E, Abraham E, Lewis SJ, Alexander D, Oxner W. Health-related quality of life following decompression compared to decompression and fusion for degenerative lumbar spondylolisthesis: a Canadian multicentre study. Can J Surg. 2014;57:E126–133.
Rosendahl K, Markestad T, Lie RT. Ultrasound screening for developmental dysplasia of the hip in the neonate: the effect on treatment rate and prevalence of late cases. Pediatrics. 1994;94:47–52.
Sewell MD, Rosendahl K, Eastwood DM. Developmental dysplasia of the hip. BMJ. 2009;339:b4454.
Sharpe P, Mulpuri K, Chan A, Cundy PJ. Differences in risk factors between early and late diagnosed developmental dysplasia of the hip. Arch Dis Child Fetal Neonatal Ed. 2006;91:F158–162.
Sponseller PD, Jain A, Shah SA, Samdani A, Yaszay B, Newton PO, Thaxton LM, Bastrom TP, Marks MC. Deep wound infections after spinal fusion in children with cerebral palsy: a prospective cohort study. Spine. 2013;38:2023–2027.
Tibrewal S, Gulati V, Ramachandran N. The Pavlik method: a systematic review of current concepts. J Pediatr Orthop B. 2013;22:516–520.
Weinstein SL. Developmental hip dysplasia and dislocation. In: Morissy RT, Weinstein SL, eds. Lovell and Winter’s Pediatric Orthopaedics. Vol 2, 5th ed. Philadelphia, PA, USA: Lippincott Williams & Wilkins; 2001:905–956.
Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2013;369:1512–1521.
Wilkinson AG, Sherlock DA, Murray GD. The efficacy of the Pavlik harness, the Craig splint and the von Rosen splint in the management of neonatal dysplasia of the hip. A comparative study. J Bone Joint Surg Br. 2002;84:716–719.
Yagi N, Hosogane M, Okada E, Watanabe K, Machida M, Tezuka M, Matsumoto M, Asazuma T, Keio Spine Research Group. Factors affecting the postoperative progression of thoracic kyphosis in surgically treated adult patients with lumbar degenerative scoliosis. Spine. 2014;39:E521–528.
Acknowledgments
We thank the Clinical Research Support Unit (CRSU) at the Child and Family Research Institute (CFRI, Vancouver, BC, Canada) for the REDCap database and study design support and expertise. We also thank the other contributing members of the IHDI study group: Peter J. Cundy, Bruce K. Foster, James R. Kasser, Young-Jo Kim, Travis H. Matheney, Colin F. Moseley, Scott J. Mubarak, Wudbhav N. Sankar, Ernest L. Sink, John H. Wedge, and Nicole Williams.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
One of the authors (KM) has received funding from the International Hip Dysplasia Institute for REDCap database coordination, maintenance, and support (http://hipdysplasia.org). Southampton work was carried out with the support of the National Institute for Health Research, Wellcome Trust Clinical Research Facility, Southampton, UK.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Included patients were recruited from all listed sites as well as Women’s and Children’s Hospital, Adelaide, Australia; Boston Children’s Hospital, Boston, MA, USA; and Children’s Hospital of Pennsylvania, Philadelphia, PA, USA. Data analysis and review were carried out at BC Children’s Hospital, Vancouver, BC, Canada.
About this article

Cite this article
Mulpuri, K., Schaeffer, E.K., Kelley, S.P. et al. What Is the Impact of Center Variability in a Multicenter International Prospective Observational Study on Developmental Dysplasia of the Hip?. Clin Orthop Relat Res 474, 1138–1145 (2016). https://doi.org/10.1007/s11999-016-4746-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-016-4746-y