
Abstract
Background
We previously reported the 5-year followup of hips with femoroacetabular impingement (FAI) that underwent surgical hip dislocation with trimming of the head-neck junction and/or acetabulum including reattachment of the labrum. The goal of this study was to report a concise followup of these patients at a minimum 10 years.
Questions/purposes
We asked if these patients had (1) improved hip pain and function; we then determined (2) the 10-year survival rate and (3) calculated factors predicting failure.
Methods
Between July 2001 and March 2003, we performed surgical hip dislocation and femoral neck osteoplasty and/or acetabular rim trimming with labral reattachment in 75 patients (97 hips). Of those, 72 patients (93 hips [96%]) were available for followup at a minimum of 10 years (mean, 11 years; range, 10–13 years). We used the anterior impingement test to assess pain and the Merle d’Aubigné-Postel score to assess function. Survivorship calculation was performed using the method of Kaplan and Meier and any of the following factors as a definition of failure: conversion to total hip arthroplasty (THA), radiographic evidence of worsening osteoarthritis (OA), or a Merle d’Aubigné-Postel score less than 15. Predictive factors for any of these failures were calculated using the Cox regression analysis.
Results
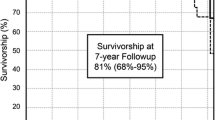
At 10-year followup, the prevalence of a positive impingement test decreased from preoperative 95% to 38% (p < 0.001) and the Merle d’Aubigné-Postel score increased from preoperative 15.3 ± 1.4 (range, 9–17) to 16.9 ± 1.3 (12–18; p < 0.001). Survivorship of these procedures for any of the defined failures was 80% (95% confidence interval, 72%–88%). The strongest predictors of failure were age > 40 years (hazard ratio with 95% confidence interval, 5.9 [4.8–7.1], p = 0.002), body mass index > 30 kg/m2 (5.5 [3.9–7.2], p = 0.041), a lateral center-edge angle < 22° or > 32° (5.4 [4.2–6.6], p = 0.006), and a posterior acetabular coverage < 34% (4.8 [3.7–5.6], p = 0.006).
Conclusions
At 10-year followup, 80% of patients with FAI treated with surgical hip dislocation, osteoplasty, and labral reattachment had not progressed to THA, developed worsening OA, or had a Merle d’Aubigné-Postel score of less than 15. Radiographic predictors for failure were related to over- and undertreatment of acetabular rim trimming.
Level of Evidence
Level IV, therapeutic study.




Similar content being viewed by others

References
Albers CE, Steppacher SD, Ganz R, Tannast M, Siebenrock KA. Impingement adversely affects 10-year survivorship after periacetabular osteotomy for DDH. Clin Orthop Relat Res. 2013;471:1602–1614.
Beaule PE, Le Duff MJ, Zaragoza E. Quality of life following femoral head-neck osteochondroplasty for femoroacetabular impingement. J Bone Joint Surg Am. 2007;89:773–779.
Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004;418:67–73.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840.
Brunner A, Horisberger M, Herzog RF. Sports and recreation activity of patients with femoroacetabular impingement before and after arthroscopic osteoplasty. Am J Sports Med. 2009;37:917–922.
Byrd JW, Jones KS. Arthroscopic management of femoroacetabular impingement: minimum 2-year follow-up. Arthroscopy. 2011;27:1379–1388.
Chiron P, Espie A, Reina N, Cavaignac E, Molinier F, Laffosse JM. Surgery for femoroacetabular impingement using a minimally invasive anterolateral approach: analysis of 118 cases at 2.2-year follow-up. Orthop Traumatol Surg Res. 2012;98:30–38.
Cox DR. Regression models and life tables. J R Stat Soc B. 1972;34:187–220.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213.
Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, Bullinger M, Kaasa S, Leplege A, Prieto L, Sullivan M. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: results from the IQOLA Project. International Quality of Life Assessment. J Clin Epidemiol. 1998;51:1171–1178.
Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001;83:1119–1124.
Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51:737–755.
Holm I, Bolstad B, Lutken T, Ervik A, Rokkum M, Steen H. Reliability of goniometric measurements and visual estimates of hip ROM in patients with osteoarthrosis. Physiother Res Int. 2000;5:241–248.
Ilizaliturri VM Jr, Orozco-Rodriguez L, Acosta-Rodriguez E, Camacho-Galindo J. Arthroscopic treatment of cam-type femoroacetabular impingement: preliminary report at 2 years minimum follow-up. J Arthroplasty. 2008;23:226–234.
Jackson TJ, Hanypsiak B, Stake CE, Lindner D, El Bitar YF, Domb BG. Arthroscopic labral base repair in the hip: clinical results of a described technique. Arthroscopy. 2014;30:208–213.
Kalberer F, Sierra RJ, Madan SS, Ganz R, Leunig M. Ischial spine projection into the pelvis: a new sign for acetabular retroversion. Clin Orthop Relat Res. 2008;466:677–683.
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–481.
Kirmit L, Karatosun V, Unver B, Bakirhan S, Sen A, Gocen Z. The reliability of hip scoring systems for total hip arthroplasty candidates: assessment by physical therapists. Clin Rehabil. 2005;19:659–661.
Larson CM, Giveans MR, Stone RM. Arthroscopic débridement versus refixation of the acetabular labrum associated with femoroacetabular impingement: mean 3.5-year follow-up. Am J Sports Med. 2012;40:1015–1021.
Laude F, Sariali E, Nogier A. Femoroacetabular impingement treatment using arthroscopy and anterior approach. Clin Orthop Relat Res. 2009;467:747–752.
Lincoln M, Johnston K, Muldoon M, Santore R. Combined arthroscopic and modified open approach for cam femoroacetabular impingement: a preliminary experience. Arthroscopy. 2009;25:392–399.
Martin RL, Sekiya JK. The interrater reliability of 4 clinical tests used to assess individuals with musculoskeletal hip pain. J Orthop Sports Phys Ther. 2008;38:71–77.
McCarthy J, Mc Millan S. Arthrocopy of the hip: factors affecting outcome. Orthop Clin North Am. 2013;44:489–498.
McWhirk LB, Glanzman AM. Within-session inter-rater realiability of goniometric measures in patients with spastic cerebral palsy. Pediatr Phys Ther. 2006;18:262–265.
Merle d’Aubigné R, Postel M. Functional results of hip arthroplasty with acrylic prostesis. J Bone Joint Surg Am. 1954;36:451–475.
Murphy S, Tannast M, Kim YJ, Buly R, Millis MB. Debridement of the adult hip for femoroacetabular impingement: indications and preliminary clinical results. Clin Orthop Relat Res. 2004;429:178–181.
Naal FD, Miozzari HH, Schar M, Hesper T, Nötzli HP. Midterm results of surgical hip dislocation for the treatment of femoroacetabular impingement. Am J Sports Med. 2012;40:1501–1510.
Naal FD, Miozzari HH, Wyss TF, Notzli HP. Surgical hip dislocation for the treatment of femoroacetabular impingement in high-level athletes. Am J Sports Med. 2011;39:544–550.
Palmer DH, Ganesh V, Comfort T, Tatman P. Midterm outcomes in patients with cam femoroacetabular impingement treated arthroscopically. Arthroscopy. 2012;28:1671–1681.
Peters CL, Schabel K, Anderson L, Erickson J. Open treatment of femoroacetabular impingement is associated with clinical improvement and low complication rate at short-term followup. Clin Orthop Relat Res. 2010;468:504–510.
Philippon MJ, Briggs KK, Yen YM, Kuppersmith DA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: minimum two-year follow-up. J Bone Joint Surg Br. 2009;91:16–23.
Reynolds D, Lucas J, Klaue K. Retroversion of the acetabulum. A cause of hip pain. J Bone Joint Surg Br. 1999;81:281–288.
Siebenrock KA, Schaller C, Tannast M, Keel M, Büchler L. Anteverting periacetabular osteotomy for symptomatic acetabular retroversion: results at ten years. J Bone Joint Surg. Epub ahead of print. DOI: 10.2106/JBJS.M.00842.
Sink EL, Leunig M, Zaltz I, Gilbert JC, Clohisy J. Reliability of a complication classification system for orthopaedic surgery. Clin Orthop Relat Res. 2012;470:2220–2226.
Steppacher SD, Huemmer C, Schwab JM, Tannast M, Siebenroc KA. Surgical hip dislocation for treatment of femoroacetabular impingement: factors predicting 5-year survivorship. Clin Orthop Relat Res. 2014;472:337–348.
Steppacher SD, Tannast M, Ganz R, Siebenrock KA. Mean 20-year followup of Bernese periacetabular osteotomy. Clin Orthop Relat Res. 2008;466:1633–1644.
Tannast M, Kakaty DK, Zheng G, Siebenrock K. What is a normal acetabulum? A computer-assisted radiographic study. In: Davies BL, Joskowicz L, Murphy SB, eds. Computer Assisted Orthopaedic Surgery. Berlin, Germany: Pro Business; 2009:254–257.
Tannast M, Mistry S, Steppacher SD, Reichenbach S, Langlotz F, Siebenrock KA, Zheng G. Radiographic analysis of femoroacetabular impingement with Hip2Norm-reliable and validated. J Orthop Res. 2008;26:1199–1205.
Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis—what the radiologist should know. AJR Am J Roentgenol. 2007;188:1540–1552.
Tönnis D. General radiography of the hip joint. In: Tönnis D, ed. Congenital Dysplasia and Dislocation of the Hip. Heidelberg, Germany: Springer-Verlag; 1987:100–142.
Ware JJ, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220–233.
Wyss TF, Clark JM, Weishaupt D, Notzli HP. Correlation between internal rotation and bony anatomy in the hip. Clin Orthop Relat Res. 2007;460:152–158.
Zahiri CA, Schmalzried TP, Szuszczewicz ES, Amstutz HC. Assessing activity in joint replacement patients. J Arthroplasty. 1998;13:890–895.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (MT) has received funding from the Swiss National Science Foundation (SNSF).
Each author certifies that he or she, or a member of their immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article

Cite this article
Steppacher, S.D., Anwander, H., Zurmühle, C.A. et al. Eighty Percent of Patients With Surgical Hip Dislocation for Femoroacetabular Impingement Have a Good Clinical Result Without Osteoarthritis Progression at 10 Years. Clin Orthop Relat Res 473, 1333–1341 (2015). https://doi.org/10.1007/s11999-014-4025-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-014-4025-8