
Abstract
Background
Current anterior fixators can close a disrupted anterior pelvic ring. However, these anterior constructs cannot create posterior compressive forces across the sacroiliac joint. We explored whether a modified fixator could create such forces.
Questions/purposes
We determined whether (1) an anterior external fixator with a second anterior articulation (X-frame) would provide posterior pelvic compression and (2) full pin insertion would deliver higher posterior compressive forces than half pin insertion.
Methods
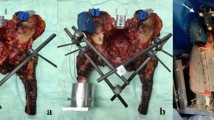
We simulated AP compression Type III instability with plastic pelvis models and tested the following conditions: (1) single-pin supraacetabular external fixator (SAEF) using half pin insertion (60 mm); (2) SAEF using full pin insertion (120 mm); (3) modified fixator with X-frame using half pin insertion; (4) modified fixator using full pin insertion; and (5) C-clamp. Standardized fracture compression in the anterior and posterior compartment was performed as in previous studies by Gardner. A force-sensitive sensor was placed in the symphysis and posterior pelvic ring before fracture reduction and the fractures were reduced. The symphyseal and sacroiliac compression loads of each application were measured.
Results
The SAEF exerted mean compressions of 13 N and 14 N to the posterior pelvic ring using half and full pin insertions, respectively. The modified fixator had mean posterior compressions of 174 N and 222 N with half and full pin insertions, respectively. C-clamp application exerted a mean posterior load of 407 N.
Conclusions
Posterior compression on the pelvis was improved using an X-frame as an anterior fixation device in a synthetic pelvic fracture model.
Clinical Relevance
This additive device may improve the initial anterior and posterior stability in the acute management of unstable and life-threatening pelvic ring injuries.


Similar content being viewed by others


References
Bachus KN, DeMarco AL, Judd KT. Measuring contact area, force, and pressure for bioengineering applications: using Fuji Film and TekScan systems. Med Eng Phys. 2006;28:483–488.
Balogh Z, King KL, Mackay P, McDougall D, Mackenzie S, Evans JA, Lyons T, Deane SA. The epidemiology of pelvic ring fractures: a population-based study. J Trauma. 2007;63:1066–1073.
Bassam D, Cephas GA, Ferguson KA, Beard LN, Young JS. A protocol for the initial management of unstable pelvic fractures. Am Surg. 1998;64:862–867.
Biau DJ, Kerneis S, Porcher R. Statistics in brief: the importance of sample size in the planning and interpretation of medical research. Clin Orthop Relat Res. 2008;466:2282–2288.
Biffl WL, Smith WR, Moore EE, Gonzalez RJ, Morgan SJ, Hennessey T, Offner PJ, Ray CE Jr, Franciose RJ, Burch JM. Evolution of a multidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. Ann Surg. 2001;233:843–850.
Burgess AR, Eastridge BJ, Young JW, Ellison TS, Ellison PS Jr, Poka A, Bathon GH, Brumback RJ. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma. 1990;30:848–856.
Cook RE, Keating JF, Gillespie I. The role of angiography in the management of hemorrhage from major fractures of the pelvis. J Bone Joint Surg Br. 2002;84:178–182.
Dalal SA, Burgess AR, Siegel JH, Young JW, Brumback RJ, Poka A, Dunham CM, Gens D, Bathon H. Pelvic fracture in multiple trauma: classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma. 1989;29:981–1000.
Day AC. Emergency management of pelvic fractures. Hosp Med. 2003;64:79–86.
DePuy Synthes Companies. Available at: http://www.depuysynthes.com. Accessed May 2008.
Dickson KF, Matta JM. Skeletal deformity after anterior external fixation of the pelvis. J Orthop Trauma. 2009;23:327–332.
DonTigny RL. Function and pathomechanics of the sacroiliac joint: a review. Phys Ther. 1985;65:35–44.
Egbers HJ, Draijer F, Havemann D, Zenker W. [Stabilizing the pelvic ring with the external fixator: biomechanical studies and clinical experiences] [in German]. Orthopade. 1992;21:363–372.
Gänsslen A, Giannoudis P, Pape HC. Hemorrhage in pelvic fracture: who needs angiography? Curr Opin Crit Care. 2003;9:515–523.
Gardner MJ, Kendoff D, Ostermeier S, Citak M, Hüfner T, Krettek C, Nork SE. Sacroiliac joint compression using an anterior pelvic compressor: a mechanical study in synthetic bone. J Orthop Trauma. 2007;21:435–440.
Gardner MJ, Nork SE. Stabilization of unstable pelvic fractures with supraacetabular compression external fixation. J Orthop Trauma. 2007;21:269–273.
Gardner MJ, Parada S, Routt ML. Internal rotation and taping of the lower extremities for closed pelvic reduction. J Orthop Trauma. 2009;23:361–364.
Ghanayem AJ, Stover MD, Goldstein JA, Bellon E, Wilber JH. Emergent treatment of pelvic fractures: comparison of methods for stabilization. Clin Orthop Relat Res. 1995;318:75–80.
Giannoudis PV, Grotz MR, Tzioupis C, Dinopolous H, Wells GE, Bouamra O, Lecky F. Prevalence of pelvic fractures, associated injuries, and mortality: the United Kingdom perspective. J Trauma. 2007;63:875–883.
Giannoudis PV, Pape HC. Damage control orthopaedics in unstable pelvic ring injuries. Injury. 2004;35:671–677.
Gilliland MD, Ward RE, Barton RM, Miller PW, Duke JH. Factors affecting mortality in pelvic fractures. J Trauma. 1982;22:691–693.
Grimm MR, Vrahas MS, Thomas KA. Pressure-volume characteristics of the intact and disrupted pelvic retroperitoneum. J Trauma. 1998;44:454–459.
Guntenberg B, Goldie I, Slätis P. Fixation of pelvic fractures and dislocations: an experimental study on the loading of pelvic fractures and sacro-iliac dislocations after external compression fixation. Acta Orthop Scand. 1978;49:278–286.
Huittinen VM, Slätis P. Postmortem angiography and dissection of hypogastric artery in pelvis fractures. Surgery. 1973;73:454–456.
Kim WY, Hearn TC, Seleem O, Mahalingam E, Stephen D, Tile M. Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res. 1999;361:237–244.
Lindahl J, Hirvensalo E, Bostman O, Santavirta S. Failure of reduction with an external fixator in the management of injuries of the pelvic ring: long-term evaluation of 110 patients. J Bone Joint Surg Br. 1999;81:955–962.
Matewski D, Szymkowiak E, Bilinski P. Analysis of management of patients with multiple injuries of the locomotor system. Int Orthop. 2008;32:753–758.
Rieger H, Winckler S, Wetterkamp D, Overbeck J. Clinical and biomechanical aspects of external fixation of the pelvis. Clin Biomech (Bristol, Avon). 1996;11:322–327.
Riemer BL, Butterfield SL, Diamond DL, Young JC, Raves JJ, Cottington E, Kislan K. Acute mortality associated with injuries to the pelvic ring: the role of early patient mobilization and external fixation. J Trauma. 1993;35:671–675.
Sadri H, Nguyen-Tang T, Stern R, Hoffmeyer P, Peter R. Control of severe hemorrhage using C-clamp and arterial embolization in hemodynamically unstable patients with pelvic ring disruption. Arch Orthop Trauma Surg. 2005;125:443–447.
Slätis P, Krarhariju EO. External fixation of the pelvic girdle with a trapezoid compression frame. Injury. 1975;7:53–56.
Slätis P, Krarhariju EO. External fixation of unstable pelvic fractures: experience in 22 patients treated with trapezoid compression frame. Clin Orthop Relat Res. 1980;151:73–80.
Solomon LB, Pohl AP, Chehade MJ, Malcolm AM, Howie DW, Henneberg M. Surgical anatomy for pelvic external fixation. Clin Anat. 2008;21:674–682.
Spanjersberg WR, Knops SP, Schep NW, van Lieshout EM, Patka P, Schipper IB. Effectiveness and complications of pelvic circumferential compression devices in patients with unstable pelvic fractures: a systematic review of literature. Injury. 2009;40:1031–1035.
Wild JJ Jr, Hanson GW, Tullos HS. Unstable fractures of the pelvis treated by external fixation. J Bone Joint Surg Am. 1982;64:1010–1020.
Acknowledgments
We thank Robert L. Garrison MD for his careful revision and Martin Schmidt MD for organization of our experiments.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he, or any member of his immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
This work was performed at the Harald Tscherne Laboratory for Trauma Research, Department of Orthopaedics/Trauma, RWTH Aachen University Hospital, Aachen, Germany.
About this article
Cite this article
Sellei, R.M., Schandelmaier, P., Kobbe, P. et al. Can a Modified Anterior External Fixator Provide Posterior Compression of AP Compression Type III Pelvic Injuries?. Clin Orthop Relat Res 471, 2862–2868 (2013). https://doi.org/10.1007/s11999-013-2993-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-2993-8