
Opinion statement
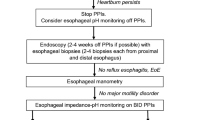
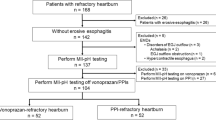
The most appropriate diagnostic and therapeutic approach to patients with heart-burn that persists despite the use of proton-pump inhibitor (PPI) therapy currently is not known. In general, patients with heartburn refractory to PPIs may have more than one explanation for their persistent symptoms. These include uncontrolled esophageal acid exposure (“PPI failure”) in a small subset of patients, as well as other potential etiologies in the majority of patients who have controlled esophageal acid exposure on PPI therapy (“PPI success”). Some potential explanations for persistent heartburn in this latter group include hypersensitivity to acid reflux, nonacidic or duodenogastric esophageal reflux, as well as functional heartburn. Patients who present with heartburn refractory to PPIs should be investigated further to determine the potential cause. We believe the diagnostic modality with the most clinical usefulness is 24-hour pH and multichannel intraluminal impedance monitoring with symptom index performed while the patient is on high-dose PPI therapy. This approach allows the patient to be properly categorized and also identifies a substantial proportion of patients who will have functional heartburn, a condition that should discourage the use of endoscopic or surgical therapies. Therapeutic options for patients with heartburn refractory to PPIs are limited and have not been thoroughly studied. As a result of the paucity of information, we favor a therapeutic approach based on the outcome of diagnostic testing.
Similar content being viewed by others

References and Recommended Reading
Locke GR 3rd, Talley NJ, Fett SL, et al.: Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmstead County, Minnesota. Gastroenterology 1997, 112:1448–1456.
Barlow WJ, Orlando RC: The pathogenesis of heartburn in nonerosive reflux disease: a unifying hypothesis. Gastroenterology 2005, 128:771–778.
Fass R, Shapiro M, Dekel R, Sewell J: Systematic review: proton-pump inhibitor failure in gastro-oesophageal reflux disease—where next? Aliment Pharmacol Ther 2005, 22:79–94.
Castell DO, Kahrilas PJ, Richter JE, et al.: Esomeprazole (40 mg) compared with lansoprazole (30 mg) in the treatment of erosive esophagitis. Am J Gastroenterol 2002, 97:575–583.
Dean BB, Gano AD, Knight K, et al.: Effectiveness of proton pump inhibitors in nonerosive reflux disease. Clin Gastroenterol Hepatol 2004, 2:656–664.
The Gallup Organization: Gallup study of consumers’ use of stomach relief products. Princeton, NJ: The Gallup Organization; 2000.
Egan LJ, Myhre GM, Mays DC, et al.: CYP2C19 pharmacogenetics in the clinical use of proton-pump inhibitors for gastro-oesophageal reflux disease: Variant alleles predict gastric acid suppression, but not oesophageal acid exposure or reflux symptoms. Aliment Pharmacol Ther 2003, 17:1521–1528.
Peghini PL, Katz PO, Bracy NA, Castell DO: Nocturnal recovery of gastric acid secretion with twice-daily dosing of proton pump inhibitors. Am J Gastroenterol 1998, 93:763–767.
Nzeako UC, Murray JA: An evaluation of the clinical implications of acid breakthrough in patients on proton pump inhibitor therapy. Aliment Pharmacol Ther 2002, 16:1309–1316.
Galmiche JP, Clouse RE, Balint A, et al.: Functional esophageal disorders. Gastroenterology 2006, 130:1459–1465.
Sgouros SN, Bergele C, Mantides A: Eosinophilic esophagitis in adults: a systematic review. Eur J Gastroenterol Hepatol 2006, 18:211–217.
Kahrilas PJ, Quigley EM: Clinical esophageal pH recording: a technical review for practice guideline development. Gastroenterology 1996, 110:1982–1996.
Tack J, Koek G, Demedts I, et al.: Gastroesophageal reflux disease poorly responsive to single-dose proton pump inhibitors in patients without Barrett’s esophagus: acid reflux, bile reflux, or both? Am J Gastroenterol 2004, 99:981–988.
Bautista JM, Wong WM, Pulliam G, et al.: The value of ambulatory 24 hr esophageal pH monitoring in clinical practice in patients who were referred with persistent gastroesophageal reflux disease (GERD)-related symptoms while on standard dose anti-reflux medications. Dig Dis Sci 2005, 50:1909–1915.
Charbel S, Khandwala F, Vaezi MF: The role of esophageal pH monitoring in symptomatic patients on PPI therapy. Am J Gastroenterol 2005, 100:283–289.
Mainie I, Tutuian R, Shay S, et al.: Acid and non-acid reflux in patients with persistent symptoms despite acid suppressive therapy. A multicentre study using combined ambulatory impedance-pH monitoring. Gut 2006, 55:1398–1402.
Fass R, Murthy U, Hayden CW, et al.: Omeprazole 40 mg once a day is equally effective as lansoprazole 30 mg twice a day in symptom control of patients with gastrooesophageal reflux disease (GERD) who are resistant to conventional-dose lansoprazole therapy-a prospective, randomized, multi-centre study. Aliment Pharmacol Ther 2000, 14:1595–1603.
Fass R, Sontag SJ, Traxler B, Sostek M: Treatment of patients with persistent heartburn symptoms: a double-blind, randomized trial. Clin Gastroenterol Hepatol 2006, 4:50–56.
Fackler WK, Ours TM, Vaezi MF, Richter JE: Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology 2002, 122:625–632.
Ours TM, Fackler WK, Richter JE, Vaezi MF: Nocturnal acid breakthrough: clinical significance and correlation with esophageal acid exposure. Am J Gastroenterol 2003, 98:545–550.
Lidums I, Lehmann A, Checklin H, et al.: Control of transient lower sphincter relaxations and reflux by the GABA (B) agonist baclofen in normal subjects. Gastroenterology 2000, 118:7–13.
Zhang Q, Lehmann A, Rigda R, et al.: Control of transient lower oesophageal sphincter relaxations and reflux by the GABA (B) agonist baclofen in patients with gastro-oesophageal reflux disease. Gut 2002, 50:19–24.
Vela MF, Tutuian R, Katz PO, Castell DO: Baclofen decreases acid and non-acid post-prandial gastrooesophageal reflux measured by combined multichannel intraluminal impedance and pH. Aliment Pharmacol Ther 2003, 17:243–251.
Koek GH, Sifrim D, Lerut T, et al.: Effect of the GABA (B) agonist baclofen in patients with symptoms of duodenogastro-oesophageal reflux refractory to proton pump inhibitors. Gut 2003, 52:1397–1402.
Degen L, Petrig C, Studer D, et al.: Effect of tegaserod on gut transit in male and female subjects. Neurogastroenterol Motil 2005, 17:821–826.
Tutuian R, Mainie I, Allan R, et al.: Effects of a 5-HT (4) receptor agonist on oesophageal function and gastro-oesophageal reflux: studies using combined impedance-manometry and combined impedance-pH. Aliment Pharmacol Ther 2006, 24:155–162.
Kahrilas PJ, Quigley EM, Castell DO, Spechler SJ: The effects of tegaserod (HTF 919) on oesophageal acid exposure in gastro-oesophageal reflux disease. Aliment Pharmacol Ther 2000, 14:1503–1509.
Rodriguez-Stanley S, Zubaidi S, Proskin HM, et al.: Effect of tegaserod on esophageal pain threshold, regurgitation, and symptom relief in patients with functional heartburn and mechanical sensitivity. Clin Gastroenterol Hepatol 2006, 4:442–450.
Prakash C, Clouse RE: Long-term outcome from tricyclic antidepressant treatment of functional chest pain. Dig Dis Sci 1999, 44:2373–2379.
Varia I, Logue E, O’Connor C, et al.: Randomized trial of sertraline in patients with unexplained chest pain of noncardiac origin. Am Heart J 2000, 140:367–372.
Gorelick AB, Koshy SS, Hooper FG, et al.: Differential effects of amitriptyline on perception of somatic and visceral stimulation in healthy humans. Am J Physiol 1998, 275:G460–G466.
Peghini PL, Katz PO, Castell DO: Imipramine decreases oesophageal pain perception in human male volunteers. Gut 1998, 42:807–813.
Broekaert D, Fischler B, Sifrim D, et al.: Influence of citalopram, a selective serotonin reuptake inhibitor, on oesophageal hypersensitivity: a double-blind, placebo-controlled study. Aliment Pharmacol Ther 2006, 23:365–370.
Arts J, Tack J, Galmiche JP: Endoscopic antireflux therapies. Gut 2004, 53:1207–1214.
Arts J, Lerut T, Rutgeerts P, et al.: A one-year follow-up study of endoluminal gastroplication (Endocinch) in GERD patients refractory to proton pump inhibitor therapy. Dig Dis Sci 2005, 50:351–356.
Campos GM, Peters JH, DeMeester TR, et al.: Multivariate analysis of factors predicting outcome after laparoscopic Nissen fundoplication. J Gastrointest Surg 1999, 3:292–300.
Swoger J, Ponsky J, Hicks DM, et al.: Surgical fundoplication in laryngopharyngeal reflux unresponsive to aggressive acid suppression: a controlled study. Clin Gastroenterol Hepatol 2006, 4:433–441.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Trivedi, A., Long, J.D. Heartburn refractory to proton-pump inhibitors. Curr Treat Options Gastro 10, 47–56 (2007). https://doi.org/10.1007/s11938-007-0056-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11938-007-0056-5