
Abstract
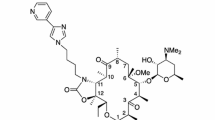
Recent surveillance studies suggest that the incidence of resistance to macrolide antibiotics in common communityacquired respiratory tract pathogens, particularly Streptococcus pneumoniae and Streptococcus pyogenes, is increasing and limiting the usefulness of these drugs. The ketolides, of which telithromycin is the first to be available for clinical use (but not yet in the United States), represent a new class of antibacterials developed specifically to combat respiratory tract pathogens that have acquired resistance to macrolides. The ketolides possess innovative structural modifications, a 3-keto group and a large N-substituted C11, C12-carbamate side chain. This novel structure allows ketolides, which are inhibitors of protein synthesis, to exert a more effective interaction with domain II of the 23S rRNA, enhancing binding to bacterial ribosomes and allowing binding to macrolide-lincosamidestreptogramin B-resistant ribosomes. This novel chemical structure also promotes greater stability of telithromycin in acid conditions, providing the potential for greater stability in gastric fluid and at cellular/tissue levels. Early clinical trials support the bacteriologic and clinical efficacy of telithromycin in the treatment of upper respiratory tract infections (RTIs) such as streptococcal pharyngitis and acute sinusitis, including infections caused by macrolide-resistant S. pneumoniae and S. pyogenes. Common adverse side effects associated with telithromycin are predominantly gastrointestinal, usually of mild to moderate severity, and rarely involve withdrawal of the drug. Telithromycin represents an attractive option for the empiric treatment of upper RTIs, especially as resistance to macrolides is likely to continue to increase.
Similar content being viewed by others


References and Recommended Reading
Zhanel GG, Hoban DJ: Ketolides in the treatment of respiratory infections. Expert Opin Pharmacother 2002, 3:277–297. This review discusses the use of ketolides in the treatment of RTI.
Zhanel GG, Dueck M, Hoban DJ, et al.: Review of macrolides and ketolides: focus on respiratory tract infections. Drugs 2001, 61:443–498. This is a comprehensive review of macrolide and ketolide mechanism of action and resistance.
Zhanel GG, Walters M, Noreddin A, et al.: The ketolides: a critical review. Drugs 2002, 62:1771–1804. This is a very detailed analysis of ketolide mechanisms of action and resistance, in vitro activity, pharmacokinetics/pharmacodynamics, and adverse effects, highlighting the differences found for macrolides.
Zhanel GG, Hisanaga T, Nichol K, et al.: Ketolides: an emerging treatment for macrolide-resistant respiratory tract infections, focusing on S. pneumoniae. Expert Opin Emerg Drugs 2003, 8:297–321. This is a comprehensive and comparative review of ketolide versus macrolide mechanism of action and resistance, pharmacokinetics/ pharmacodynamics, clinical trials, and adverse effects.
Bryskier A: Ketolides-telithromycin, an example of a new class of antibacterial agents. Clin Microbiol Infect 2000, 6:661–669.
Capobianco JO, Cao Z, Shortridge VD, et al.: Studies of the novel ketolide ABT-773: transport, binding to ribosomes, and inhibition of protein synthesis in Streptococcus pneumoniae. Antimicrob Agents Chemother 2000, 44:1562–1567.
Ban N, Nissen P, Hansen J, et al.: The complete atomic structure of the large ribosomal subunit at 2.4 A resolution. Science 2000, 289:905–920.
Champney WS, Tober CL: Structure-activity relationships for six ketolide antibiotics. Curr Microbiol 2001, 42:203–210.
Champney WS, Tober CL: Superiority of 11,12 carbonate macrolide antibiotics as inhibitors of translation and 50S ribosomal subunit formation in Staphylococcus aureus cells. Curr Microbiol 1999, 38:342–348.
Novotny GW, Andersen NM, Poehlsgaard J: Telithromycin interacts directly with the base of A752 in domain II of 23S ribosomal RNA, in contrast to erythromycin and clarithromycin [abstract P480]. In 11th European Congress of Clinical Microbiology and Infectious Diseases. Istanbul, Turkey: 2001.
Hansen LH, Mauvais P, Douthwaite S: The macrolide-ketolide antibiotic binding site is formed by structures in domains II and V of 23S ribosomal RNA. Mol Microbiol 1999, 31:623–631.
Douthwaite S, Mauvais P, Champney WS, Bryskier A: Structureactivity relationship of the ketolide telithromycin (HMR 3647) [abstract 02.02]. In 5th International Conference on the Macrolides, Azalides, Streptogramins, Ketolides, and Oxazolidinones. Seville, Spain: 2000.
Douthwaite S, Hansen LH, Mauvais P: Macrolide-ketolide inhibition of MLS-resistant ribosomes is improved by alternative drug interaction with domain II of 23S rRNA. Mol Microbiol 2000, 36:183–193.
Roberts MC, Sutcliffe J, Courvalin P, et al.: Nomenclature for macrolide and macrolide-lincosamide-streptogramin B resistance determinants. Antimicrob Agents Chemother 1999, 43:2823.
Tait-Kamradt A, Davies T, Appelbaum PC, et al.: Two new mechanisms of macrolide resistance in clinical strains of Streptococcus pneumoniae from Eastern Europe and North America. Antimicrob Agents Chemother 2000, 44:3395–3401.
Tait-Kamradt A, Davies T, Cronan M, et al.: Mutations in 23S rRNA and ribosomal protein L4 account for resistance in pneumococcal strains selected in vitro by macrolide passage. Antimicrob Agents Chemother 2000, 44:2118–2125.
Bonnefoy A, Girard AM, Agouridas C, Chantot JF: Ketolides lack inducibility properties of MLS(B) resistance phenotype. J Antimicrob Chemother 1997, 40:85–90.
Mauvais P, Bonnefoy A: Lack of in vitro MLSB resistance induction by the ketolide telithromycin (HMR 3647): role of the 3-keto group [abstract 02.10]. In 5th International Conference on the Macrolides, Azalides, Streptogramins, Ketolides, and Oxazolidinones. Seville, Spain: 2000.
Perret C, Lenfant B, Weinling E, et al.: Pharmacokinetics and absolute oral bioavailability of an 800-mg oral dose of telithromycin in healthy young and elderly volunteers. Chemotherapy 2002, 48:217–223.
Odenholt I, Lowdin E, Cars O: Pharmacodynamics of telithromycin: in vitro against respiratory tract pathogens. Antimicrob Agents Chemother 2001, 45:23–29.
Sultan E, Namour F, Mauriac C, et al.: The ketolide antimicrobial, telithromycin (HMR 3647), is metabolized and eliminated predominantly in the faeces in man [abstract 09.31]. In 5th International Conference on the Macrolides, Azalides, Streptogramins, Ketolides, and Oxazolidinones. Seville, Spain: 2000.
Sharma K, Katgely B, Villa R, Pluim J: Safety profile of the first ketolide antimicrobial, telithromycin: a review [abstract P17.018]. In 22nd International Congress of Chemotherapy. Amsterdam, The Netherlands: 2001.
Zhanel GG, Neuhauser M: The ketolides. In Antimicrobial Agents. Edited by Yu V, McKinnon N. New York: Lippincott, Williams and Wilkins; 2004, In press. This is a ketolide review with great emphasis on drug-drug interaction, adverse side effects, effects of disease states and host immunity, and brief indications for treatment of upper and lower RTIs.
Bisno AL, Gerber MA, Gwaltney JM Jr, et al.: Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Infectious Diseases Society of America. Clin Infect Dis 2002, 35:113–125.
Betriu C, Casado MC, Gomez M, et al.: Incidence of erythromycin resistance in Streptococcus pyogenes: a 10-year study. Diagn Microbiol Infect Dis 1999, 33:255–260.
Norrby S, Rabie W, Bacart P, et al.: Efficacy of 5 days’ telithromycin (HMR 3647) vs 10 days’ penicillin V in the treatment of pharyngitis in adults [abstract 2242]. Paper presented at the 40th Interscience Conference on Antimicrobial Agents and Chemotherapy. Toronto, Canada, September 17–20, 2000.
Chang J, Stewart J, Brumpt I, et al.: Telithromycin (HMR 3647) provides more rapid relief from symptoms than penicillin V in patients with GABHS pharyngitis [abstract P1262]. In 11th European Congress of Clinical Microbiology and Infectious Diseases. Istanbul, Turkey: 2001.
Quinn J, Ziter P, Leroy B, et al.: Oral telithromycin (HMR 3647) 800 mg once daily for 5 days is well tolerated and as effective as oral clarithromycin 250 mg twice daily for 10 days in group A-hemolytic streptococcal (GABHS) pharyngitis/ tonsillitis [abstract 2229]. Paper presented at the 40th Interscience Conference on Antimicrobial Agents and Chemotherapy. Toronto, Canada, September 17–20, 2000.
Roos K, Brunswig-Pitschner C, Kostrica R, et al.: Efficacy and tolerability of a 5-day course of a new ketolide antimicrobial, telithromycin (HMR 3647), for the treatment of acute sinusitis [abstract 2243]. Paper presented at the 40th Interscience Conference on Antimicrobial Agents and Chemotherapy. Toronto, Canada, September 17–20, 2000.
Buchanan P, McNeil D, Tady D, et al.: A 5-day course of telithromycin, the first ketolide antibacterial, is as effective as 10 days cefuroxime axetil in the treatment of acute maxillary sinusitis [abstract 910]. In 41st Interscience Conference on Antimicrobial Agents and Chemotherapy. Chicago: 2001.
Tellier G, Lasko B, Leroy B, et al.: Oral telithromycin (HMR 3647) 800 mg once daily for 5 days and 10 days is well tolerated and as effective as amoxicillin/clavulanic acid 500/125 mg three times daily for 10 days in acute maxillary sinusitis (AMS) in adults [abstract 2226]. Paper presented at the 40th Interscience Conference on Antimicrobial Agents and Chemotherapy. Toronto, Canada, September 17–20, 2000.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Zhanel, G.G., Wierzbowski, A.K., Hisanaga, T. et al. The use of ketolides in treatment of upper respiratory tract infections. Curr Infect Dis Rep 6, 191–199 (2004). https://doi.org/10.1007/s11908-004-0008-3
Issue Date:
DOI: https://doi.org/10.1007/s11908-004-0008-3