
Abstract
The Maptaphut industrial area, one of the largest petrochemical complexes in Thailand, is the major cause of the various air pollutants. The larger concern is that a significant volume of air pollution is emitted and that air quality management needs to be improved. This is in part due to a lack of deeper understanding of how anthropogenic emissions are emitted from different sources in this area— especially volatile organic compounds (VOCs). Moreover, it has complicated relationship results of air pollution, disease mechanisms, and health effects. As a result, its available data can only give a rough indication of them. These factors are often assumed to be associated with economic consequences, but assessing the health-related economic losses caused by air pollution remains limited in many ways.
Four targeted VOCs were analyzed, including benzene, 1,3-butadiene, 1,2-dichloroethane, and vinyl chloride from industrial and non-industrial sources, namely stacks, flares, storage tanks, wastewater treatment plants, transportation and marketing, fugitive losses, slurry/open equipment/vessel, and on-road mobile emissions. Source apportionment can be conducted using emissions inventory (EI) to establish pollution source databases, the dispersion model, and then imported on the risk model by determining receptors. The AERMOD dispersion model coupled with the IRAP-h view model was used to predict the spatial distribution of the ground-level concentration and analyze the inhalation health risk covering cancer and non-cancer risks— as well as the prioritization of pollutants.
The risk assessment results indicated that the highest risk occurred most from 1,3-butadiene for cancer and chronic non-cancer risks contributed to fugitive sources, about 83% and 94%, and most benzenes for acute non-cancer risk contributed to on-road mobile sources, at about 56%.
Consequently, the benzene classified as the most important priority depending on its risk results, comprehensive epidemiological studies, and discharge volumes.
With the economic benefits assessment, BenMAP-CE was further utilized to estimate the health impacts and economic value of multiple scenarios to facilitate decision-making for benzene reduction. Overall, the 10% rollback policy for benzene concentration, monetized value of about 13.13 billion US dollars for all mortalities, gave the best practical scenario for the most economically viable option based on the B/C (benefit/cost) ratio results in Maptaphut. Ultimately, policymakers need to take additional measures to improve air quality and reduce health impacts while also considering economic benefits, especially benzene reduction.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Air pollution significantly affects the health of humans, especially in the urban industrial area (Khan and Ghouri 2011; Gong et al. 2015). It also has a substantial economic impact by increasing medical expenses, and reducing productivity through the loss of working days across the economic sector (EEA 2018; Tsai et al. 2019). Exposure to air pollution contributes to an estimated seven million premature deaths globally each year, mostly in low-income and middle-income countries (WHO 2021). Moreover, air pollution cost an estimated 8.1 trillion dollars in 2019, which is 6.1 percent of the global GDP (World Bank 2022). Thus, it is evident why the impacts of air pollution on human health and the consequent social costs have received more attention and have become a global issue (Tsai et al. 2019).
The Maptaphut industrial area (MA) is the largest chemical and petrochemical complex in Thailand (Chusai et al. 2012), this is due to industrial and infrastructure development projects under the eastern economic corridor (EEC) plan in Thailand. As a consequence, the GDPs of the industrial sector has been increased. On the other hand, it is one of the notorious industries for air pollution-related illnesses, especially volatile organic compounds (VOCs) (Tanyanont and Vichit-Vadakan 2012). Monitored data of temporal variations in VOC concentrations in the Maptaphut industrial area have found that VOCs exceeded the national air quality standard each year in several monitoring stations, namely benzene; 1,3-butadiene; 1,2-dichloroethane; vinyl chloride (PCD 2018). The cause of concern is that air quality management in the area is complex, partly because of a need to understand how anthropogenic emissions from different sources or sectors play a role in air quality control (Chusai et al. 2012). They were supposed to be released and were expected to migrate from industrial sources, the most significant contributors to its, especially petrochemical complexes (Baltrėnas et al. 2011; Hsu et al. 2018; Zheng et al. 2019) and non-industrial sources in the ambient air (Jia et al. 2012), such as cleaning products in households, chemical facilities, combustion process, gasoline exhaust emissions from traffic, and gas vapor from the gas stations (Liu et al. 2008; Zhang et al. 2014; Saeaw and Thepanondh 2015; Hsu et al. 2018; Jia et al. 2022) as well as most Hazardous air pollutants (HAPs) belong to VOCs (Tsai 2016). They affect the chemistry of the atmosphere (Hsu et al. 2018), and have toxic and carcinogenic human health effects (Li et al. 2020). Exposure to VOCs can cause long-term and short-term effects (Tanyanont and Vichit-Vadakan 2012). VOCs can cause residents living in the vicinity of a petrochemical industrial complex to have health risks to target organ systems, e.g., respiratory, blood, liver, kidney, and central nervous system —and cause a series of adverse reactions, especially cancer in the human body (Stander 2000; Niu et al. 2014; USEPA 2017a).
Unfortunately, the MA has complex issues in terms of air pollution, disease mechanisms, and health effects; as a result, the available data can only give a rough indication— despite the unnaturally high number of some cancers (Thepanondh et al. 2011). As for the statistics of diseases at the regional level, from 1998 to 2012, it was found that the incidence of leukemia in Rayong province was higher than at the national level, which may be related to VOCs in Mapthaphut —which could lead to mortality and mobility (DDC 2020). Although this information is limited by the lack of epidemiological studies on whether it is related to specific-compound pollution in Thailand (DDC 2020), the suspect was benzene (identified as a group I) because it can also cause leukemia (IARC 1997).
Epidemiological studies indicated that benzene, a key component in petrochemical processes (Chen et al. 2016), was identified as the highest cancer risk and can also lead to the development of lymphocyte cell reduction, thrombocytopenia (Jung et al. 2012), and leukemia (Kirkeleit et al. 2008; Khalade et al. 2010; Snyder 2012; Hsu et al. 2018), while butadiene was associated with an increased risk of non-Hodgkin lymphoma (Sathiakumar et al. 1998). Furthermore, empirical evidence has been widely published on the target organ for chronic exposure to benzene in the hematologic system, and for acute exposure target organs are hematologic, immune, and reproductive systems (Mirrezaei and Orkomi 2020; OEHHA 2015; Yoon et al. 2018). Hence, the relevant agencies have vigorously tried to control emissions (Boonyanam 2016).
However, it is noticed that there is growing evidence of epidemiological research on a relationship between air pollution and respiratory illness and mortality (Briggs et al. 1997), and these factors are often assumed to be related to economic value (Sacks et al. 2018), but also a lack of assessment of health-related economic losses caused by air pollution, —which has become a hot topic nowadays (Li et al. 2016). Because the agencies often do not have the potentiality or resources to conduct original valuation research, especially in the conceptions of benefits transfer are employed to find similar policy contexts that allow for dollar values to be applied to changes in the incidence or prevalence of health outcomes in Thailand (USEPA 2012; Sacks et al. 2018).
This study pioneers the utilization of BenMap-CE as a novel approach to assess the presence of VOCs in the Thai region. Previous investigations have not explored this specific application. By employing BenMap-CE, an advanced computational tool, the research seeks to unravel intricate insights into the intricate nexus between VOC exposure and its potential health ramifications within the context of Thailand. The study's pioneering nature underscores its significance in expanding the scientific understanding of VOC-related health impacts, thus contributing to the formulation of data-driven strategies for effective risk management.
Thus, this study determined the emission inventory (EI) of VOCs emitted by both industrial and non-industrial sources in MA. Four VOC species of carcinogenic pollutants: benzene, 1,3-butadiene, 1,2-dichloroethane, and vinyl chloride, were selected as the targeted VOCs of the study. The AERMOD model was applied to demonstrate their spatial concentration and used for plot files in subsequent risk assessments. The IRAP-h view was also conducted to evaluate the extent of exposure to each substance for the potential health risks to prioritize the VOC species. Finally, BenMAP-CE was used to assess the potential health impacts, considered the first attempt to apply its beta coefficients that quantitatively characterize the relationship between air pollution exposure and health effects of specific VOCs in Thailand, and the economic benefits of changes in air quality for formulating appropriate and effective policies pragmatically for the protection of public health in the Maptaphut industrial area. The findings and methodology demonstrated in this study can be a protocol for Maptaphut or other studies.
Method
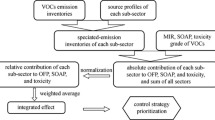
The sequential process for forecasting air concentrations, evaluating health risks, prioritizing VOCs, and quantifying health benefits in the Maptaphut region is depicted in Fig. 1. This progression commences with the collection of VOC measurements, establishment of EIs, followed by air and risk prediction, determination of source contributions, culminating in the analysis of health benefits.

Overview of the study design
Study area
The study focused on the Maptaphut industrial area (MA) of the Rayong province in eastern Thailand. It has been announced as a pollution control area by the Thai government since 2009 (ONEP 2009). Currently, it consists of five industrial estates, namely Map Ta Phut, East Hemaraj, Asia, Padaeng, and RIL industrial estates, and one deep-sea port (Fig. 1). Its processes can be divided into two basic categories: upstream and midstream based on petrochemical products. In addition, there are various factories in MA, including petrochemical, coal-fired power plants, iron and steel, natural gas power plants, gas separation plants, and oil refineries (ONEP 2016). These factories are the contributors to local and regional VOCs in the ambient air. Moreover, VOCs can be fugitive as they may be derived from other sources, e.g., transportation in this area. As a result, VOCs are released into the atmosphere, a health threat that people in the area constantly face.
Ambient VOCs concentration data
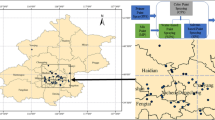
VOCs including benzene, 1,3-butadiene, 1,2-dichloroethane, and vinyl chloride, were subjected to measurement for their concentration data. These measurements were procured from an extensive network of ambient air monitoring stations, comprising 21 distinct stations, utilizing available data spanning the time frame of 2012 to 2019. As the data quality varied between stations, the inclusion of specific data was based on the following criteria. Missing data of VOCs were replaced by the geometric mean of their VOCs in each monitoring site; however, if any substance had missing data more significant than 25%, their targeted VOCs were not considered. Consequently, the entirety of the data encompassing all four compounds designated for analysis originates exclusively from the records of 16 air quality monitoring stations specifically for the year 2019 (Fig. 2).

Location of the study area, source, and air quality monitoring station
Sampling and analysis of VOCs
Sampling and analysis of the samples were following U.S. EPA Compendium Method TO-15 under QA/QC, and ISO/IEE 17025 procedures, which does identify performance criteria for whole air canister sampling, which used 6-L evacuated canisters (stainless-steel-polished) on passive sampling with 24-h measurements via sub-atmospheric pressure and VOC analyzed by gas chromatograph/mass spectrophotometer (GC/MS) with cryogenic preconcentration. Prior to use, canister samplers must be verified as free of any contamination. Cleaned and preset ultra-low flow orifices for each ambient air sample preset by the laboratory at a flow rate of 3.47 mL/min. Before each sampling with a canister, a blank sample (zero air) was analyzed to ensure that the concentration of all compounds inside was below 0.02 ppbv. The blank shall be tested at least 10 times and should be less than the limit of detection (LOD), estimated from the mean of the blank. Duplicate sampling and trip blanks should be done in at least 10% of all samples, replicating precision within 25 percent. For those compounds detected in blanks, the method detection limit (MDL) and the method limit of quantification (MQL) were computed by multiplying the standard deviation of field blank (trip or travel blanks) values by three and ten, respectively. MDL was determined for each compound and ranged from 0.04 to 0.10 (µg/m3), as shown in Table 1. The calibration curve must be linear with an R2 value of at least 0.99. Daily calibration checks should not deviate from the calibration curve by over 20% (PCD 2008). Further intricacies of the sampling and analytical procedures are expounded upon in prior works by Thepanondh et al. (2011); Saikomol et al. (2019); Jindamanee et al. (2020); Pinthong et al. (2022). The concentrations measured across the designated study sites have been subjected to comprehensive analysis and are elucidated through the utilization of descriptive statistical methods, as outlined in Table 2. These data not only serve as a crucial empirical foundation for our investigation but also function as the cornerstone of a baseline scenario depicting the air quality surface under consideration.
AERMOD
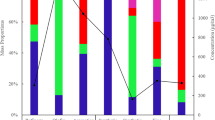
AERMOD View (version 9.9.0, Lakes Environmental Software, Waterloo, Ontario, Canada) was used to predict the spatial distribution of VOC concentration values and to discriminate the source contribution of exposure to each pollutant in receptors. Details of the configuration were designed as follows: UTM zone 47 N (m) of X (easting): 732768 and Y(northing): 1409232, cover an area of 12.5 × 12.5 km2, No. of points: x = 50 m; y = 50 m, Grid spacing: x = 500 m; y = 500 m, Length: x = 24,500 m; y = 24,500 m. Meteorological data files (surface and profile) are used for prognostic data for 2019. The terrain data were obtained from the global digital elevation model (DEM) from high-resolution NASA’s Shuttle Radar Topography Mission (SRTM) with a horizontal resolution of 90 m. The identification of discrete cartesian receptors was established through the selection of 16 out of the 21 air monitoring stations, guided by the criterion of having comprehensive data availability (completeness). This its outcome is illustrated in Fig. 2. Discrete cartesian receptors were determined from 16 air monitoring stations based on the availability (completeness) of all comprehensive monitoring stations, as shown in Fig. 1. As for source emission, the distinct VOCs emission in this area focused on two major sources, which consisted of industrial activities of each source, namely stack and flare emissions, leakage from storage tanks, wastewater, transportation and marketing, and fugitive emissions as well as slurry/open equipment/vessel (SOV), and non-industrial sources from on-road mobile emission. This study used the recent five years to substitute the incomplete data on the latest year of emission inventory (EI) on behalf of the Industrial Estate Authority of Thailand (IEAT) to identify and estimate industrial source emissions. For on-road transportation, emission line sources data comprised of 11 roads based on emission factors and related parameters from other studies (Thepanondh 2012; Thawonkaew et al. 2016). Unfortunately, the number of vehicles data are available only on two (R11 and R12) highways retrieved from the Bureau of Highway Safety (BHS) in 2019. Meanwhile, other roads are calculated from the annual growth rate based on the 2013 database of Thepanondh (2012). The two main types of VOC emissions are benzene and 1,3-butadiene. Source apportionment can be carried out using EI to establish pollution source databases as its auxiliary. After that, the dispersion model was applied to create source groups for various types of each source and then provide designated receptors that can quantify the average contribution of different sources by calculating ambient concentrations at specific locations as interested (e.g., measuring stations) to achieve apportionment results by a percentage (Lai et al. 2019). Characterization of model parameters was as input data as point, area, and line sources (Fig. 2). Figure 3 showed the proportion of source structures based on anthropogenic VOCs emissions when imported into the air model for sources parameterization. The modeling area was the largest source (50%), with the most contribution from the fugitive sources (22%). According to the EI in 2019, the emission of benzene was 78.89 ton yr−1, 1,3-butadiene was 13.15 ton yr−1, 1,2-dichloroethane was 7.72 ton yr−1, and vinyl chloride was 37.78 ton yr−1 in MA, illustrated in more detail in Malakan et al. (2022) (Table S1). The output plot files as inputs to the risk modeling contain modeled concentrations of all receptor points on the unitized emission.

Proportion of source structures based on anthropogenic VOCs emissions
IRAP-h view
The main objective of the risk model is to quantify both chronic (cancer and non-cancer risks) and acute exposures associated with all targeted VOCs for estimating the probability of adverse health impact of air pollution on people exposed. The risk assessment modeling was based on the U.S. EPA Region 6 Human Health Risk Assessment Protocol (HHRAP) (USEPA 2005). Model output plot files were interpolated from AERMOD via fate and transport algorithms as inputs to the risk modeling. In this study, potential carcinogenic and non-carcinogenic inhalation risks were automatically calculated in a comprehensive IRAP-h view risk assessment model (version 5.1.0, Lakes Environmental Software, Waterloo, Ontario, Canada) by comparing the predicted media concentration (\({\text{C}}_{i}\)) of the annual average value for chronic exposure and 1-h maximum value for acute exposure in air through generic equation with the inhalation unit risk (IUR), reference concentration (RfC), and acute inhalation exposure criteria (AIEC). These values are available in the COPC (chemicals of potential concern) properties database of IRAP-h View, which provides references that follow the U.S. EPA-approved hierarchy, illustrated, and described in more detail in Malakan et al. (2022). The health risk assessment assumed that VOCs remain as only a vapor phase (Fraction of volatilization = 1.0) for potential exposure. Therefore, only the inhalation pathway was designated for the significant exposure route. After that, the risk and hazard results were considered to select the most severe pollutants for both short-term and long-term inhalation and used further to assess their economic value from changes in air quality. Most importantly, accessible data on those substances must be available for estimating health impact, particularly the beta coefficient from an air pollution epidemiologic study for further steps. In this case, benzene was selected. In addition, the risk exposure display of all receptors is unnecessary to minimize computational time and demonstrate results more efficiently, and therefore, only the results of some crucial receptors are shown in all risks and hazards. Therefore, the selected two locations are the grid nodes with the highest risk and the lowest risk receptors, to demonstrate which VOCs and sources are of priority.
BenMAP—CE
The Environmental Benefits Mapping and Analysis Program (BenMAP-CE, version 1.5.8, U.S. EPA) was used to characterize and estimate the potential health impacts and economic benefits of the changes in air quality. It needs three principal processes to perform an analysis: 1) create an air quality surface; 2) estimate health impact; 3) monetize health benefits (USEPA 2012; Ding et al. 2016). The input data and processes were used in the analysis as follows:
Air quality data of benzene concentration
BenMAP requires both the baseline (business as usual) and control (expected air quality levels reflect the change in air quality after the policy intervention) scenarios to estimate the effects of a change in air quality (delta). Establishing air quality surfaces can be conducted using either modeled or observed values. Therefore, it is imperative for this study to meticulously ascertain the reliability and precision of input data, accurately representing authentic emission sources. Consequently, observed concentrations were employed within the baseline scenario to mitigate uncertainties and facilitate the execution of BenMAP. Conversely, predicted concentrations were computed through prior air and risk models, enabling the prioritization of pollutants and the assessment of source apportionments. The connection between measurements and the AEROMOD model lies in the fact that the measured VOC concentrations collected from canister samples serve as valuable input data for the model. The model then uses this data, along with meteorological and emission source information, to simulate how VOCs disperse in the atmosphere, helping to estimate the concentration levels at various locations and times. This integrated approach allows for a better understanding of how VOCs behave in the environment and their potential impact on air quality. As seen in Table 2, annual average benzene concentrations measured in 2019 were retrieved from PCD (Pollution Control Department) and IEAT (Industrial Estate Authority of Thailand) for each air station within industrial and community zones — which ranged between 1.03—8.43 μg/m3. We also applied spatial interpolation by using Voronoi neighbor averaging (VNA) in the GIS to estimate ambient benzene concentration and to create a continuous surface in an unmonitored area for a specific distance of each village in MA from neighboring monitors, as shown in Fig. 4.

Air quality surface based on rollback algorithm to Thai annual standard for (a) Baseline scenario, (b) Control scenario, and (c) Delta (the difference between baseline and control air quality data)
Air pollution rollback scenarios
BenMAP provides predefined “rollback” or “decrement” strategies to reduce benzene concentrations to improve air quality and to protect against the potential health impact of exposure to benzene pollution (Carvour et al. 2018; Sacks et al. 2018). We considered additional policy scenarios assuming alternative counterfactual concentrations of percentage rollback, incremental rollback, and rollback-to-a-standard. In this study, 11 distinct rollbacks were employed as control scenarios. Each scenario involved the implementation of an air pollution control plan tailored to adhere to specific benchmarks, encompassing background concentrations, the annual benzene standard, and the 24-h surveillance value applicable to both Thailand and Israel. Remarkably, these standards were selected to compare between two countries because they used the same index for the averaging interval period pertaining to both 24-h and annual standards within the Asian context, despite differences in the specific numerical values. Additionally, the Environmental Performance Indicator (EPI) program of New Zealand (Ministry for the Environment of New Zealand, 2020) was integrated into the analysis under certain reasonable assumptions. These assumptions were informed by the following elucidation: the utilization of existing Thailand National Ambient Air Quality Standards (NAAQS) for VOCs; selection of the most stringent standard for Israel, identified among available sources, as conducted by Sekar et al. (2019); and the incorporation of widely recognized air quality categories as a percentage for New Zealand was guided by adherence to regional criteria. Our objective was to assess whether Thailand should contemplate the adoption of more stringent monitoring values based on the most stringent standard or opt for a gradual reduction in concentration (e.g., percentage). This evaluation is crucial, as the implementation of stringer policies can exert a considerable impact on budgets allocated for air quality management and adaptation. They comprised of 1.7 incremental rollback, 95, 70, 50, 25 and 10% rollbacks, and rollback to 24-h and annual concentration of global best and Thai standards as well as best-case scenario rollback (background) — and then determine the most suitable strategy through benefit/cost ratio. This study provides an example of air quality surface based on rollback to Thai annual standard between (a) pre-policy; valued ≤ 1.56 to > 5.49 μg/m3 and (b) post-policy; valued ≤ 1.27 to > 1.70 μg/m3, as well as (c) the difference between the two scenarios; valued ≤ 0.11 to > 3.79 μg/m3, as shown in Fig. 4.
Exposed population
Population datasets in BenMAP can assess the health impact for different groups classified by age, gender, race, and ethnicity. The total population, including workers and residents, was recruited, and used to represent the exposed population without classification due to the lack of available demographic variables in this study, similar to Ding et al. (2016). The number of registered inhabitants who expected air pollution exposures within the boundaries of 38 communities of Maptaphut Municipality was 68,546 villagers obtained from the Bureau of registration admission BORA (2019). In addition, the number of registered workers in the Map Ta Phut Industrial Estate was obtained from the Department of industrial works 7,209 (DIW, 2021). Thus, the total population in this study was 75,755. The population distribution is based on the original data by a spatially weighted average approach to generate different grid definition levels over a defined geographic extent, as illustrated in Fig. 5.

Population distribution over the study area, 2019
Mortality data
This protocol adheres to the regulations stipulated by the “Research with Exemption” ethical review committee for human research, denoted as No. 6/2565, which enabled the acquisition of statistical data, including mortality and morbidity rates. This data was sourced from local and provincial governmental entities, notably the hospital unit in Rayong, through the Health Data Center (HDC) of Thailand for the year 2019, as documented by the Ministry of Public Health in 2019. In fact, doctors currently have relatively few code records in diagnosing diseases caused by environmental pollution because of the low number of physicians specializing in environmental medicine in Thailand. Moreover, the available data is the overall illness data from all causes only, and illness information is difficult to access. In addition, the mechanism of disease caused by environmental pollution exposure is complex (DDC 2020), but fortunately, the mortality data were recorded in the annual report. Therefore, the health endpoints were selected based on the published literature for deaths associated with benzene toxicity to determine the health impact. The mortality rate, or baseline incidence rate, used for the analysis represents the total number of deaths per year in the study area and classified the cause of death according to the ICD-10 (International Classification of Diseases) code for 6 health endpoints (Table 3). To reduce bias from an underestimation of leukemia mortality, more benzene-related mortality data may be available but not recorded in hospitals under Health Service Network 6 of the local government scale; therefore, the provincial level is used instead during the same year.
Estimation of health impacts
The health impact functions (HIFs) in BenMAP-CE were used to estimate health impacts, which utilize air-quality data, population data, baseline incidence rates, and concentration–response (C-R) relationships—which can be calculated from a simple algebraic Eq. (1), resulting from changes in benzene concentration-related mortality (USEPA 2017b). For the above reasons, no epidemiological studies have limited domestic research in Thailand on selected volatile organic compounds associated with cause-specific mortality, especially benzene. Hence, this study carefully reviewed previous epidemiological studies, particularly those from Asia, with a focus on South Asia. This process involves systematically combining and synthesizing findings to derive comprehensive insights to identify relative risks since populations are expected to share similarities to Thai populations (Nandar et al. 2020) and to result in specific concentration–response coefficients (beta values), as shown in Table 4 for almost all health endpoints except for cancer and lung cancer deaths from Toronto, North America.
where: ΔY is the estimated health impact attributed to air pollution or the number of avoided premature deaths as a result of an air quality improvement; β is the C-R coefficient (beta coefficient), which is calculated from relative risk reported in the reliable epidemiological reference through ln (RR; Relative risk) / ΔAQ and then imported it into the software; ΔAQ is the change in benzene concentration to some target or health standard value, 1.7 was used based on Thai annual standard; Yo is baseline incidence rate for each health effect (Table 4); and Pop is population exposed to air pollution.
Economic valuation of health impacts
To estimate the economic value of changes in the incidence of health effects, we used a country-specific value of statistical life (VSL), which is the rate at which people are willing to pay for a reduction in their risk of premature death, to calculate the benefits of mortality risk reductions in monetary values (Dockins et al. 2004; Lindhjem et al. 2011). The VSL can be estimated in Eq. (2) for converting a U.S. VSL in U.S. dollars in 2013 to a Thai VSL in baht of 2019.
where: \({VSL}_{TH, 2019}\) is the VSL value for Thailand in 2019 in units of Thai baht (THB) per statistical death per year; \({VSL}_{US, 2013}\) is the VSL value for U.S. in 2013 of 8,662,172 U.S. Dollar (USD), which is mean VSL in current dollars were used in this study from USDA, Economic Research Service; \(Y\) is the GDP per capita of the specified country in the specified year for TH, 2019 of 19,233.86 and US, 2013 of 53,106.54 international (PPP-adjusted) dollars (World Bank, International Comparison Program database); ε is the income elasticity of the VSL (the percentage increase in VSL for a percentage increase in income) used BenMAP default of 0.4; \({PPP}_{TH, 2013}\) is the purchasing power parity conversion factor in 2013 used 12.3 Thai baht per International Dollar; and \({CPI}_{TH}\) is the consumer price index for Thailand in 2013 of 109.27 and 2019 of 113.26 (World Bank 2021).
Health benefit
To estimate the health benefits of avoided health effects as a result of improving alternative ambient air quality standards, the economic value was estimated by the following Eq. (3):
where: \({V}_{i}\) is the economic value of avoiding a single case of a particular health effect (U.S. Dollars); \({\Delta Y}_{i}\) is the impact for health endpoint i; and \({C}_{i}\) is the benefit value or cost of health effect per case (value of statistical life (VSL) or cost of illness (COI)). In the study, we estimate monetized benefits by using VSL.
Result and Discussion
Air dispersion modeling
As shown in Fig. 6, the spatial distribution of annual concentration indicated that the predicted concentrations of all four targeted pollutants did not exceed their annual national standard for all receptor sites. The highest concentration of all targes occurred within the fence line in the Map Ta Phut industrial estate and closer to the road due to their source congestion, especially benzene and 1,3-butadiene that were considered as markers of the petrochemical industry (Pinthong et al. 2022), while 1,2-dichloroethane and vinyl chloride concentrations were attributed to the manufacturing of the polyvinylchloride plastic (Randall 1994; Garcia-Herrero et al. 2017). However, the observed concentrations were used as input data to estimate the health impacts and economic value because of greater reliability.

Spatial distribution of predicted annual concentration of (a) benzene, (b) 1,3-butadiene, (c) 1,2-dichloroethane, and (d) vinyl chloride
Health risk and hazard
Cancer risk
The cancer risk for each VOC was higher than the acceptable standard (1 × 10–5) based on the U.S. EPA Region 6 in all receptors, even the lowest-risk receptor, as shown in Fig. 7. The total cancer risk contributed by for all VOCs of inhalation exposure reached 3.91 × 10–1 for adults and 7.82 × 10–2 for children at the highest carcinogenic risk receptor. The elevated risk surpasses expectations, signifying that individuals face a probability as high as 4 in 10 for adults and 8 in 100 for children, throughout their lifetimes, of developing cancer due to the contemplated exposure. This event occurred closer to the industrial (Map Ta Phut and RIL industrial estates) and non-industrial (highway due to its high traffic volume) sources (Tsai et al. 2019), was mainly caused by 1,3-butadiene (2.87 × 10–1 for adults and 5.75 × 10–2 for children) from the fugitive source about 83% of total cancer risk as shown in Fig. 8a. Hence, there is a necessity for implementing corrective measures to mitigate the potential risk. However, within the context of risk assessment in Thailand, it is crucial to acknowledge the absence of established standards currently. Consequently, it becomes imperative for Thai policymakers to recognize the importance of evaluating calculated risks and, in response, to implement more stringent measures. We recommend that they proactively establish comprehensive risk assessment protocols and standards tailored to the specific needs of Thailand.

Cancer risk of (a) the highest risk receptor and (b) the lowest risk receptor

Percentage children and adults at the highest risk of (a) Cancer (b) Chronic non-cancer, and (c) Acute non-cancer
Non-cancer hazard
Non-cancer hazards or hazard quotients (HQs) were divided by VOC according to key receptors mentioned earlier, as shown in Table 5. The analysis revealed that, in comparison to a standard exposure level and considering all receptors in both children and adults, the chronic and acute Hazard Quotients (HQs) for nearly all substances were found to exceed the non-cancer benchmark value of 0.25, with the exception of 1,2-dichloroethane. Whose health effects might include the reproductive, blood, and liver systems according to organ effects database. In the context of the hazard index (HI), it was determined that the combined presence of all VOCs led to the exceeding of the non-cancer benchmark, established by the U.S. EPA Region 6 (HHRAP), for all receptors encompassing resident children and adults. This observation implies the potential occurrence of non-cancerous health effects. Moreover, the highest HI for chronic inhalation of 6.38 × 103 and acute inhalation of 2.53 × 102, which occurred in the same location as the carcinogenic result, was mainly attributed to 1,3-butadiene from the fugitive source of about 94% of total chronic non-cancer risk (Fig. 8b) and benzene from on-road mobile source about 56% of total acute non-cancer risk as (Fig. 8c), respectively. This result is similar to the work of Sadeghi-Yarandi et al. (2020) and Khajeh Hoseini et al. 2022 that increased cancer and non-cancer risks were attributed to benzene and 1,3-butadiene, respectively.
However, it is attributed to different organ endpoints, considered biased results from the organ effects database because the HI should be based on the same target system and target organ (Adams et al. 2017). Moreover, the potential human health risk from chronic exposure via direct inhalation of vapor was considered as a conservative approach as they do not take into account the time spent indoors where particulates tend to settle out and not be inhaled, but it calculates the exposure at the receptor location based on continuous exposure to the outdoor air concentration— which might overestimate prediction even though we have already accounted for time spent away from the point of maximum unitized air concentrations (USEPA 2005). As for acute HQ, results are no wonder that the value exceeded the acceptable standard because excessive one-hour peak concentrations of all receptors resulted in predicted acute hazard values being overestimated (Rood 2014; Kumar et al. 2017).
The results of the study indicated that government agencies should be reducing non-cancer and cancer risks, especially 1,3-butadiene and benzene, which are the first two priorities, followed by vinyl chloride and 1,2-dichloroethane, respectively. However, there are no definitive studies on human reproductive effects after inhalation of 1,3-butadiene (ATSDR 1992; Choudhary 1994) according to the risk model. Regardless of 1,3-butadiene, although its long-term carcinogenic risk can occur in humans (Gao et al. 2022). This study, therefore, chose to assess the health impact and economic value of benzene because of its more complete epidemiological evidence and where maximum discharge volume—which is considered the priority that should be controlled caused by stationary sources, and port activities as well as vehicle sources in Maptaphut petroleum and petrochemical industrial estate (WHO 2010; Thepanondh et al. 2011; Tsai et al. 2019).
BenMap-CE
No concrete information on the reproductive or developmental effects of 1,3-butadiene in humans is available. Therefore, only benzene was evaluated in this study.
Health burden
Figure 9 and Table S2 presented the avoided mortalities for 6 mortality endpoints under different scenario reduction of benzene based on reporting unrounded figures to substantiate the consistency of the results as described in Sacks et al. (2018) The results showed that a rollback to the best-case scenario (background concentration) enables the achievement of the most significant reduction in aggregating premature deaths, about 41 cases per year of total health endpoints, most of whom die from cancer in the entire Maptaphut industrial area. Pragmatically, this scenario was considered an ideal situation and was quite tricky to implement potentially. However, even with the reduction of benzene at low concentrations, it still has harmful health impacts (Bolden et al. 2015). Meanwhile, a rollback to Thai 24-h surveillance has not changed significantly in preventable premature deaths since benzene annual mean concentrations at most stations were less than 7.6 µg/m3. According to percentile, avoided deaths in circulatory and leukemia for all scenario reductions is more accurate and reliable because their percentiles are not negative. However, negative percentiles in other mortality endpoints did not mean that they were unreliable and negligible, but it could potentially be more reflected in statistical uncertainty in the study, as shown in Table S2. Thus, the decrease in air pollutant concentrations can reduce the mortality rate, which brings considerable economic value (Liu 2022).

Avoidable deaths for different air quality reduction from annual ambient benzene concentration
Economic benefits
The results in Fig. 10 indicated that a rollback to the best-case scenario could reduce the monetary value of all mortalities up to 99.02 billion US dollars. As for individual health endpoints, avoidable cancer mortality (C01—C97) could reduce the monetary value that an individual is most willing to exchange for reductions in risk of death, approximately 1.29—57.27 billion US dollars (Table S3). This is because benzene and overall cancer have a relatively strong relationship (Villeneuve et al. 2013). Consequently, benzene-related deaths are attributed to malignant neoplasms (cancerous tumors) based on local hospital databases and concurred with Yin et al. (1989). Moreover, benzene was related to hematopoietic and leukemia mortalities (Yin et al. 1989; Rinsky et al. 2002). This study gives two examples of economic value after a 10% rollback for circulatory and leukemia in the Maptaphut area, as shown in Fig. 11.

Economic benefit after benzene reduction

Monetized values after implementing a 10% rollback due to (a) Circulatory, and (b) Leukemia
Benefit/Cost ratio (B/C ratio)
The results in Table 6 indicated that a 10% rollback policy, monetized value for all mortalities was about 13.13 billion US dollars (4.06 hundred million Thai baht), can be considered a sustainable option and the most economically viable (B/C = 0.084 and 6.57) for the Thai government's policy because it gives the highest B/C in all cases for both central and local budget management. Moreover, the number of monetized values was six times higher compared to those obtained based on values from a rollback to Thai 24-Hr surveillance, which was the second most economically viable (B/C = 0.083 and 6.52). Therefore, this strategy should be implemented.
Uncertainties and limitations
As for the air and risk models, the meteorological data files, and the emissions inventory (EI) must have a certain degree of accuracy in order to be less uncertain. The potential human health risk assessment was considered a conservative approach (worst-case scenario) and used constant emissions, which may be overestimated. With regard to BenMap-CE, mortality data had general limitations regarding the specificity of mortality in each community. As a result, the calculated incidence rates were generalized to the entire Maptaphut Municipality instead of a specific community for finer resolution. Nevertheless, provincial premature deaths were used for leukemia. The VNA algorithm was used to remediate the lack of VOC monitoring stations in all community and industrial areas. To determine the background concentrations of benzene, the lowest value was used from the 16 monitoring stations in Rayong for 2019. Regarding the health impact function, the beta value was taken from extensive literature reviews based on the relative risk of Asia to avoid regional differences and particularities of individual studies as much as possible—except for cancer and lung cancer from North America due to insufficient domestic research. Even though other specified personal risk factors (e.g., sex, smoking, alcohol intake, income, other health conditions, medications) are adjusted parameters or not, so there can be uncertainty because it does not belong directly to the local people (Kwon et al. 2018). Conducting a Monte Carlo analysis, the study sought to derive a comprehensive estimation encompassing a spectrum of health effects. This was achieved by generating specific percentiles, ranging from the 2.5th to the 97.5th percentile, thereby capturing a diverse array of potential health outcomes. The outcomes of this analysis are comprehensively detailed in Supplementary Table S2. For VSL, income elasticity is not applied to middle-income countries (Thailand); instead, a default value is used. Elasticity should use 0.9 for Thailand. Further studies are needed to decrease their uncertainty for greater accuracy. However, this study provides a sensitivity analysis of many parameters that could affect health endpoint over a range of reasonable values and specially created site-specific beta coefficient. It does not cover all of the morbidity and mortality related to benzene. Additional health endpoints (Hematopoietic mortality, Neurological morbidity, etc.) should be evaluated in future work.
Conclusion
Four VOC species of carcinogenic pollutants: benzene, 1,3-butadiene, 1,2-dichloroethane, and vinyl chloride, were selected as the targeted VOCs of the study. The AERMOD was simulated to determine the spatial characteristics of VOC concentrations and used their plot files in subsequent risk assessments. IRAP-h was performed to assess potential inhalation health risks and to prioritize specific pollutants. The results indicated that the predicted annual-average concentrations of all four targeted pollutants did not exceed the annual standard for all receptor sites by AERMOD, which provided less accurate results than observed concentrations. Thus, measured concentrations from 16 monitoring sites were used as input data for baseline air quality conditions to ensure the data entry accuracy and reduce the uncertainty to run BenMAP-CE.
The inhalation cancer risks of all targeted VOCs were within the unacceptable risk levels at both residential and industrial areas. As for non-carcinogenic inhalation, both acute and chronic effects were also higher than the acceptable levels, except for 1,2-dichloroethane. Based on the highest risk receptor, 1,3-butadiene and benzene were evaluated as the most contributing emission source of fugitive losses for cancer risk and chronic HQ, as well as on-road vehicle sources for acute HQ, respectively. Thus, corrective and preventive actions are needed to protect the resident population from them in terms of cancer and non-cancer risks.
With empirically epidemiological evidence and risk results, benzene was diagnosed as the most important priority. To strengthen the evidence-based estimates and embark on efforts in Thailand for supporting integrated health impact through literature review, the various potential beta coefficients of benzene were applied to derive specific health impact functions.
As for potential policy options, the proposal to minimize benzene concentration as the best-case scenario resulted in the avoidance of 41 premature deaths (monetized value 99.02 billion US dollars) with a monetary cost ranging from 0.02 to 1.50 billion US dollars. However, this approach may not be deemed appropriate in practice. Conversely, a marginal reduction in concentration as the worst-case scenario, based on the Thai 24-h surveillance value, yielded negligible changes in health burden (monetized value 2.16 billion US dollars) and a monetary cost ranging from 0.03 to 2.48 ten million US dollars.
The benefit/cost ratio indicated that reducing the concentration to only 10 percent emerges as the most suitable policy for stringent economic regulation, resulting in the prevention of approximately 5 health cases with a monetized value of about 13.13 billion US dollars. The associated monetary cost for this policy ranges from 0.19 to 14.95 ten million US dollars.
This research protocol is consistent with the principles of all for health in the overall planning of the EEC area, which leads to the industrial development of empirical data on health and policy with respect to emission control of policy analysts and decision-makers. In addition, research helps stakeholders recognize the impact of its programs in response to the Sustainable Development Goals (SDGs) for sustainable socio-economic and environmental development. Thus, leading to initiate, improve, and inform public health and air quality policies in Thailand. However, further epidemiological investigation and economic benefits attributed to other health endpoints should be taken.
Data availability
The data presented in this study are available in supplementary material.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Adams VH, McAtee MJ, Johnson MS (2017) Implementation of the basic hazard index screening for health risks associated with simultaneous exposure to multiple chemicals using a standardized target organ and systems framework. Integr Environ Assess Manag 13(5):852–860. https://doi.org/10.1002/ieam.1899
ATSDR (Agency for Toxic Substances and Disease Registry) (1992) Toxicological Profile for 1,3-Butadiene. Available at: https://www.atsdr.cdc.gov/toxprofiles/tp28.pdf. Public Health Service, U.S. Department of Health and Human Services, Atlanta, GA. Accessed 13 Mar 2021
Baltrėnas P, Baltrėnaitė E, Šerevičienė V, Pereira P (2011) Atmospheric BTEX concentrations in the vicinity of the crude oil refinery of the Baltic region. Environ Monit Assess 182:115–127. https://doi.org/10.1007/s10661-010-1862-0
Bolden AL, Kwiatkowski CF, Colborn T (2015) New look at BTEX: Are ambient levels a problem? Environ Sci Technol 49(9):5261–5276. https://doi.org/10.1021/es505316f
Boonyanam N (2016) Loss of Value in House Properties due to Air Pollution in Map Ta Phut Industrial Area of Thailand. Appl Environ Res 38(3):1–13. https://doi.org/10.35762/AER.2016.38.3.1
BORA (Bureau of registration admission) (2019) Official statistics registration systems, Demographic statistics. Available online: https://www.bora.dopa.go.th/index.php/th/. Accessed 11 Mar 2021
Briggs DJ, Collins S, Elliott P, Fischer P, Kingham S, Lebret E, Pryl K, VanReeuwijk H, Smallbone K, VanDerVeen A (1997) Mapping urban air pollution using GIS: a regression-based approach. Int J Geogr Inf Sci 11(7):699–718. https://doi.org/10.1080/136588197242158
Carvour ML, Hughes AE, Fann N, Haley RW (2018) Estimating the health and economic impacts of changes in local air quality. Am J Public Health 108(S2):S151–S157. https://doi.org/10.2105/AJPH.2017.304252
Chen MJ, Lin CH, Lai CH, Cheng LH, Yang YH, Huang LJ, Yeh SH, Hsu HT (2016) Excess lifetime cancer risk assessment of volatile organic compounds emitted from a petrochemical industrial complex. Aerosol Air Qual Res 16(8):1954–1966. https://doi.org/10.4209/aaqr.2015.05.0372
Choudhary G (1994) Environmental exposure to 1, 3-butadiene: A human health perspective. J Environ Sci Health C 12(1):23–61. https://doi.org/10.1080/10590509409373429
Chusai C, Manomaiphiboon K, Saiyasitpanich P, Thepanondh S (2012) NO2 and SO2 dispersion modeling and relative roles of emission sources over Map Ta Phut industrial area. Thailand J Air Waste Manag Assoc 62(8):932–945. https://doi.org/10.1080/10962247.2012.687704
DDC (Department of Disease Control) 2020 Report on environmental and health situations in the Eastern Special Development Zone. Bangkok, Thailand.
Ding D, Zhu Y, Jang C, Lin CJ, Wang S, Fu J, Gao J, Deng S, Xie J, Qiu X (2016) Evaluation of health benefit using BenMAP-CE with an integrated scheme of model and monitor data during Guangzhou Asian Games. J Environ Sci 42:9–18. https://doi.org/10.1016/j.jes.2015.06.003
DIW (Department of industrial works) (2021) Factory information in the Industrial Estate Authority of Thailand. Available online: http://userdb.diw.go.th/factory/ieat.asp. Accessed 23 Mar 2021
Dockins C, Maguire K, Simon N, Sullivan M (2004) Value of statistical life analysis and environmental policy: A white paper. U.S. Environmental Protection Agency Press, National Center for Environmental Economics
EEA (European Environment Agency) (2018) Air quality in Europe - 2018 report. Denmark, Copenhagen
Gao S, Zhang Z, Wang Q et al (2022) Emissions and health risk assessment of process-based volatile organic compounds of a representative petrochemical enterprise in East China. Air Qual Atmos Health 15:1095–1109. https://doi.org/10.1007/s11869-021-01117-4
Garcia-Herrero I, Margallo M, Laso J, Onandía R, Irabien A, Aldaco R (2017) Measuring the vulnerability of an energy intensive sector to the EU ETS under a life cycle approach: the case of the Chlor-Alkali industry. Sustainability 9(5):837. https://doi.org/10.3390/su9050837
Gong J, Hu Y, Liu M, Bu R, Chang Y, Li C, Wu W (2015) Characterization of Air Pollution Index and Its Affecting Factors in Industrial Urban Areas in Northeastern China. Pol J Environ Stud 24(4):1579. https://doi.org/10.15244/pjoes/37757
Hsu CY, Chiang HC, Shie RH, Ku CH, Lin TY, Chen MJ, Chen NT, Chen YC (2018) Ambient VOCs in residential areas near a large-scale petrochemical complex: Spatiotemporal variation, source apportionment and health risk. Environ Pollut 240:95–104. https://doi.org/10.1016/j.envpol.2018.04.076
IARC (International Agency for Research on Cancer) 1997 IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans ‘Benzene’ 29:93–148, 391–398. Lyon, France.
Jia C, Batterman SA, Relyea GE (2012) Variability of indoor and outdoor VOC measurements: an analysis using variance components. Environ Pollut 169:152–159. https://doi.org/10.1016/j.envpol.2011.09.024
Jia C, Fu X, Chauhan B et al (2022) Exposure to volatile organic compounds (VOCs) at gas stations: a probabilistic analysis. Air Qual Atmos Health 15:465–477. https://doi.org/10.1007/s11869-021-01124-5
Jindamanee K, Thepanondh S, Aggapongpisit N, Suktawee S (2020) Source apportionment analysis of volatile organic compounds using positive matrix factorization coupled with conditional bivariate probability function in the industrial areas. EnvironmentAsia 13:31–49. https://doi.org/10.14456/ea.2020.28
Jung JH, Choi BW, Kim MH, Baek SO, Lee GW, Shon BH 2012 The characteristics of the appearance and health risks of volatile organic compounds in industrial (Pohang, Ulsan) and non-industrial (Gyeongju) areas. Environ Health Toxicol 27. https://doi.org/10.5620/eht.2012.27.e2012012
Khajeh Hoseini L, Jalilzadeh Yengejeh R, Mohammadi Rouzbehani M, Sabzalipour S (2022) Health risk assessment of volatile organic compounds (VOCs) in a refinery in the southwest of Iran using SQRA method. Front Public Health 10:978354. https://doi.org/10.3389/fpubh.2022.978354
Khalade A, Jaakkola MS, Pukkala E, Jaakkola JJ 2010 Exposure to benzene at work and the risk of leukemia: a systematic review and meta-analysis. Environ Health 9(31). https://doi.org/10.1186/1476-069X-9-31
Khan MA, Ghouri AM (2011) Environmental pollution: its effects on life and its remedies. Res World: J Arts Sci Commer 2(2):276–285
Kirkeleit J, Riise T, Bråtveit M, Moen BE (2008) Increased risk of acute myelogenous leukemia and multiple myeloma in a historical cohort of upstream petroleum workers exposed to crude oil. Cancer Causes Control 19:13–23. https://doi.org/10.1007/s10552-007-9065-x
Kumar A, Patil RS, Dikshit AK, Kumar R (2017) Application of WRF model for air quality modelling and AERMOD-a survey. Aerosol Air Qual Res 17(7):1925–1937. https://doi.org/10.4209/aaqr.2016.06.0265
Kwon JW, Park HW, Kim WJ, Kim MG, Lee S 2018 Exposure to volatile organic compounds and airway inflammation. Environ Health 17(65). https://doi.org/10.1186/s12940-018-0410-1
Lai HC, Ma HW, Chen CR, Hsiao MC, Pan BH (2019) Design and application of a hybrid assessment of air quality models for the source apportionment of PM2. 5. Atmos Environ 212:116–127. https://doi.org/10.1016/j.atmosenv.2019.05.038
Li C, Li Q, Tong D, Wang Q, Wu M, Sun B, Su G, Tan L (2020) Environmental impact and health risk assessment of volatile organic compound emissions during different seasons in Beijing. J Environ Sci 93:1–12. https://doi.org/10.1016/j.jes.2019.11.006
Li L, Lei Y, Pan D, Yu C, Si C 2016 Economic evaluation of the air pollution effect on public health in China’s 74 cities. Springerplus 5(402). https://doi.org/10.1186/s40064-016-2024-9
Lindhjem H, Navrud S, Braathen NA, Biausque V (2011) Valuing mortality risk reductions from environmental, transport, and health policies: A global meta-analysis of stated preference studies. Risk Anal: Int J 31(9):1381–1407. https://doi.org/10.1111/j.1539-6924.2011.01694.x
Liu H (2022) Health depreciation effect and medical cost effect of air pollution: based on multidimensional health perspective. Air Qual Atmos Health 15:877–892. https://doi.org/10.1007/s11869-022-01189-w
Liu Y, Shao M, Lu SH, Chang CC, Wang JL, Fu L (2008) Source apportionment of ambient volatile organic compounds in the Pearl River Delta, China: Part II. Atmos Environ 42(25):6261–6274. https://doi.org/10.1016/j.atmosenv.2008.02.027
Malakan W, Thepanondh S, Kondo A (2022) Modeling of Inhalation Health Risk of Volatile Organic Compounds in the Vicinity of Maptaphut Petroleum and Petrochemical Industrial Estate. Thail Sustain 14(19):12073. https://doi.org/10.3390/su141912073
Ministry for the Environment of New Zealand (2020) Ambient Air Quality Guidelines. Available online: https://environment.govt.nz/assets/Publications/Files/ambient-guide-may02.pdf. Accessed 10 Mar 2022
Ministry of Public Health (2019) Report of death classified by cause of death for 298 disease groups (hospital base), Health region 6, Rayong. Available online: https://hdcservice.moph.go.th. Bangkok, Thailand.
Mirrezaei MA, Orkomi AA (2020) Gas flares contribution in total health risk assessment of BTEX in Asalouyeh. Iran Process Saf Environ 137:223–237. https://doi.org/10.1016/j.psep.2020.02.034
Nandar SL, Bonnet S, Garivait S, Thao PT (2020) Assessment of health benefits using BenMAP-CE in Myanmar. J Sustain Energy Environ 11:123–129
Niu ZG, Xu SY, Gong QC (2014) Health risk assessment of odors emitted from urban wastewater pump stations in Tianjin, China. Environ Sci Pollut Res 21:10349–10360. https://doi.org/10.1007/s11356-014-2984-7
OEHHA (Office of Environmental Health Hazard Assessment) 2015 Air Toxics Hot Spots Program Risk Assessment Guidelines; Technical Support Document for Exposure Assessment and Stochastic Analysis. California.
ONEP (Office of Natural Resources and Environmental Policy and Planning) 2009 Pollution controlled zone in 2009. Bangkok, Thailand.
ONEP (Office of Natural Resources and Environmental Policy and Planning) 2016 Emission sources data in Map Ta Phut area for air modeling. Bangkok, Thailand.
PCD (Pollution Control Department) 2008 Guide to Analysis of Volatile Organic Compounds in ambient air using with using specially prepared canisters. Air Quality and Noise Management Bureau. Bangkok, Thailand.
PCD (Pollution Control Department) 2018 Thailand state of pollution report 2018. Bangkok, Thailand.
Pinthong N, Thepanondh S, Kondo A (2022) Source identification of VOCs and their environmental health risk in a petrochemical industrial area. Aerosol Air Qual Res 22:210064. https://doi.org/10.4209/aaqr.210064
Ran J, Qiu H, Sun S, Tian L (2018) Short-term effects of ambient benzene and TEX (toluene, ethylbenzene, and xylene combined) on cardiorespiratory mortality in Hong Kong. Environ Int 117:91–98. https://doi.org/10.1016/j.envint.2018.04.049
Randall PM (1994) Pollution prevention strategies for the minimizing of industrial wastes in the VCM-PVC industry. Environ Prog 13:269–277. https://doi.org/10.1002/ep.670130416
Rayong Provincial Public Health Office (2019) Report on the number of deaths classified by cause of death for 103 disease groups. Rayong, Thailand
Rinsky RA, Hornung RW, Silver SR, Tseng CY (2002) Benzene exposure and hematopoietic mortality: A long-term epidemiologic risk assessment. Am J Ind Med 42(6):474–480. https://doi.org/10.1002/ajim.10138
Rood AS (2014) Performance evaluation of AERMOD, CALPUFF, and legacy air dispersion models using the Winter Validation Tracer Study dataset. Atmos Environ 89:707–720. https://doi.org/10.1016/j.atmosenv.2014.02.054
Sacks JD, Lloyd JM, Zhu Y, Anderton J, Jang CJ, Hubbell B, Fann N (2018) The Environmental Benefits Mapping and Analysis Program-Community Edition (BenMAP–CE): A tool to estimate the health and economic benefits of reducing air pollution. Environ Modell Softw 104:118–129. https://doi.org/10.1016/j.envsoft.2018.02.009
Sadeghi-Yarandi M, Karimi A, Ahmadi V, Sajedian AA, Soltanzadeh A, Golbabaei F (2020) Cancer and non-cancer health risk assessment of occupational exposure to 1, 3-butadiene in a petrochemical plant in Iran. Toxicol Ind Health 36(12):960–970. https://doi.org/10.1177/074823372096223
Saeaw N, Thepanondh S (2015) Source apportionment analysis of airborne VOCs using positive matrix factorization in industrial and urban areas in Thailand. Atmos Pollut Res 6(4):644–650. https://doi.org/10.5094/APR.2015.073
Saikomol S, Thepanondh S, Laowagul W (2019) Emission losses and dispersion of volatile organic compounds from tank farm of petroleum refinery complex. J Environ Health Sci Eng 17:561–570. https://doi.org/10.1007/s40201-019-00370-1
Sathiakumar N, Delzell E, Hovinga M, Macaluso M, Julian JA, Larson R, Cole P, Muir D (1998) Mortality from cancer and other causes of death among synthetic rubber workers. Occup Environ Med 55(4):230–235. https://doi.org/10.1136/oem.55.4.230
Sekar A, Varghese GK, Varma MR 2019 Analysis of benzene air quality standards, monitoring methods and concentrations in indoor and outdoor environment. Heliyon 5(11). https://doi.org/10.1016/j.heliyon.2019.e02918
Snyder R (2012) Leukemia and benzene. Int J Environ Res Public Health 9(8):2875–2893. https://doi.org/10.3390/ijerph9082875
Stander LH (2000) Regulatory aspects of air pollution control in the United States. In: Davis WT (ed) Air Pollution Engineering Manual, 2nd edn. New York, NY, USA, JohnWiley & Sons, pp 8–21
Tantiwat W, Gan C, Yang W (2021) The Estimation of the Willingness to Pay for Air-Quality Improvement in Thailand. Sustainability 13(21):12313. https://doi.org/10.3390/su132112313
Tanyanont W, Vichit-Vadakan N (2012) Exposure to volatile organic compounds and health risks among residents in an area affected by a petrochemical complex in Rayong. Thail Se Asian J Trop Med 43(1):201
Thawonkaew A, Thepanondh S, Sirithian D, Jinawa L (2016) Assimilative capacity of air pollutants in an area of the largest petrochemical complex in Thailand. Int J GEOMATE 11(23):2162–2169
Thepanondh S (2012) Development of emission factors for air pollutants and greenhouse gases from vehicle for establishment of appropriate mitigation policy and measure in the transportation sector in Thailand. Faculty of Public Health, Mahidol University, Department of Sanitary Engineering
Thepanondh S, Varoonphan J, Sarutichart P, Makkasap T (2011) Airborne volatile organic compounds and their potential health impact on the vicinity of petrochemical industrial complex. Water Air Soil Pollut 214:83–92. https://doi.org/10.1007/s11270-010-0406-0
Tsai WT (2016) Toxic volatile organic compounds (VOCs) in the atmospheric environment: regulatory aspects and monitoring in Japan and Korea. Environ 3(3):23. https://doi.org/10.3390/environments3030023
Tsai JH, Gu WT, Chung I, Chiang HL (2019) Airborne air toxics characteristics and inhalation health risk assessment of a metropolitan industrial complex. Aerosol Air Qual Res 19(11):247–2489. https://doi.org/10.4209/aaqr.2019.08.0422
USEPA (2005) Human Health Risk Assessment Protocol (HHRAP) for Hazardous Waste Combustion Facilities (Final), EPA530-R-05–006. Office of Solid Waste and Emergency Response, Washington DC, US
USEPA (2012) Environmental Benefits Mapping and Analysis Program - Community Edition User's Manual. Available at: http://www.epa.gov/airquality/benmap/models/BenMAPManualOct2012.pdf. Accessed 13 Jan 2021
USEPA (2017a) Environmental Benefits Mapping and Analysis Program - Community Edition User’s Manual. Available online: https://www.epa.gov/sites/production/files/2015-04/documents/benmap-ce_user_manual_march_2015.pdf. Accessed 12 May 2022
USEPA (2017b) Volatile Organic Compounds’ Impact on Indoor Air Quality. Available online: https://www.epa.gov/indoor-air-quality-iaq/volatile-organic-compounds-impact-indoor-air-quality. Accessed 13 June 2022
Villeneuve PJ, Jerrett M, Su J, Burnett RT, Chen H, Brook J, Wheeler AJ, Cakmak S, Goldberg MS (2013) A cohort study of intra-urban variations in volatile organic compounds and mortality, Toronto, Canada. Environ Pollut 183:30–39. https://doi.org/10.1016/j.envpol.2012.12.022
Weng HH, Tsai SS, Chiu HF, Wu TN, Yang CY (2008) Association of childhood leukemia with residential exposure to petrochemical air pollution in Taiwan. Inhal Toxicol 20(1):31–36. https://doi.org/10.1080/08958370701758734
WHO (2010) Exposure to benzene: A major public health concern. Geneva 27, Switzerland.
WHO (2021) New WHO Global Air Quality Guidelines aim to save millions of lives from air pollution. Air Pollution is One of the Biggest Environmental Threats to Human Health, Alongside Climate Change. Available online: https://www.who.int/news/. Accessed 5 May 2022
World Bank (2022) The Global Health Cost of PM2.5 Air Pollution : A Case for Action Beyond 2021. International Development in Focus;. Washington, DC: World Bank.
World Bank (2021) Data Bank: World DevelopmentIndicators. Available online: https://databank.worldbank.org/reports.aspx?source=world-development-indicators. Accessed on Feb 2021
Yin SN, Li GL, Tain FD, Fu ZI, Jin C, Chen YJ et al (1989) A retrospective cohort study of leukemia and other cancers in benzene workers. Environ Health Perspect 82:207–213. https://doi.org/10.1289/ehp.8982207
Yoon JH, Kwak WS, Ahn YS (2018) A brief review of relationship between occupational benzene exposure and hematopoietic cancer. Ann Occup Environ Med 30(33). https://doi.org/10.1186/s40557-018-0245-9
Zhang J, Sun Y, Wu F, Sun J, Wang Y (2014) The characteristics, seasonal variation and source apportionment of VOCs at Gongga Mountain, China. Atmos Environ 88:297–305. https://doi.org/10.1016/j.atmosenv.2013.03.036
Zheng H, Kong S, Yan Y, Chen N, Yao L, Liu X, Wu F, Cheng Y, Niu Z, Zheng S, Zeng X, Yan Q, Wu J, Zheng M, Liu D, Zhao D, Qi S (2019) Compositions, sources and health risks of ambient volatile organic compounds (VOCs) at a petrochemical industrial park along the Yangtze River. Sci Total Environ 135505. https://doi.org/10.1016/j.scitotenv.2019.135505
Acknowledgements
The authors greatly appreciate the support with emission and concentration data from the Pollution Control Department (PCD) and the Industrial Estate Authority of Thailand (IEAT), the community boundaries from Maptaphut Municipality, the number of deaths from the Thai Ministry of Public Health. This research project is supported by National Research Council of Thailand (NRCT) [No. NRCT5-RGJ63012-136]. This research work was supported in part by the grant from Center of Excellence on Environmental Health and Toxicology (EHT), OPS, Ministry of Higher Education, Science, Research and Innovation, Faculty of Public Health, Mahidol University, Thailand.
Funding
Open access funding provided by Mahidol University. This research project is supported by National Research Council of Thailand (NRCT) [No. NRCT5-RGJ63012-136].
Author information
Authors and Affiliations
Contributions
All the authors contributed to the study conception and design.
Conceptualization, supervision, editing, and reviewing were performed by Sarawut Thepanondh and Wissawa Malakan. Data curation, methodology designing, and investigation were performed by Sarawut Thepanondh, Jutarat Keawboonchu, Vanitchaya Kultan, Akira Kondo, and Hikari Shimadera; formal analysis was performed by Wissawa Malakan, Jutarat Keawboonchu, and Vanitchaya Kultan; writing of original draft and validation were performed by Wissawa Malakan, Akira Kondo, and Hikari Shimadera. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Institutional review board statement
The aforementioned project has been reviewed and ap-proved according to the Standard Operating Procedures of the Ethical Review Committee for Human Research, Faculty of Public Health, Mahidol University. This protocol complies with a “Research with Exemption” category (No. 6/2565).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Malakan, W., Thepanondh, S., Keawboonchu, J. et al. Integrated assessment of inhalation health risk and economic benefit of improving ambient targeted VOCs in Petrochemical industrial area. Air Qual Atmos Health (2024). https://doi.org/10.1007/s11869-024-01552-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11869-024-01552-z