
Abstract
Background
Early cardiac death is more common in patients with Crohn’s disease (CD) than in healthy adults, but the exact cause is unknown.
Aims
The aim of this study is to investigate the cardiac magnetic resonance imaging (MRI) findings in patients with CD and compare the MRI findings with healthy controls (HCs). This study also aimed to demonstrate the possible cardiac involvement in patients with CD using MRI.
Methods
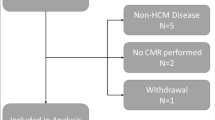
In this prospective study, participants with CD (n = 20) and HC (n = 20) underwent cardiac MRI. Erythrocyte sedimentation rate (ESR) and hematocrit levels were investigated before MRI in both groups. Two observers evaluated the ventricular functional and morphological parameters in consensus. Myocardial T1/T2-relaxation times were calculated by two observers independently using two different software, and hematocrit-corrected left ventricle extracellular volume (LV-ECV) was calculated. Observer-2 also performed histogram analysis for T1/T2-mapping images.
Results
Patients with CD had a significantly higher LV-ECV, mildly decreased right ventricle ejection fraction, and prolonged T2-relaxation time than HC. Moreover, histogram analysis showed that the maximum and mean T2-relaxation times were higher in patients with CD. There was an excellent agreement between observers for the assessment of mean native and post-contrast T1-relaxation time (intraclass correlation coefficient (ICC) of 0.991 and ICC of 0.941, respectively) and mean T2-relaxation time measurements (ICC of 0.983). Moreover, mean T2-relaxation time was found to be significantly correlated with ESR.
Conclusions
This study suggests visually undetectable myocardial involvement due to chronic systemic inflammation in patients with Crohn’s disease. Cardiac MRI can help assess and monitor cardiac involvement in patients with CD.




Similar content being viewed by others


Abbreviations
- MRI:
-
Magnetic resonance imaging
- LV:
-
Left ventricle
- RV:
-
Right ventricle
- LVEF:
-
Left ventricular ejection fraction
- WBC:
-
White blood cell
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
- BTFE:
-
Balanced turbo field echo
- sBTFE:
-
Sine balanced turbo field echo
- BBSSh:
-
Black blood single shot
- T2 STIR:
-
T2-short tau inversion recovery
- PSIR:
-
Phase-sensitive inversion recovery
- TF:
-
Turbo factor
- FA:
-
Flip angle
- FOV:
-
Field of view
- Slice Thic.:
-
Slice thickness.
- ECV:
-
Extracellular volume
- Min:
-
Minimum
- Max:
-
Maximum
- Skew:
-
Skewness
- Kurt:
-
Kurtosis
- AUC:
-
Area under the curve
- CI:
-
Confidence interval
- CD:
-
Crohn’s disease
References
Torres J, Mehandru S, Colombel J, Peyrin-Biroulet L (2017) Crohn’s disease. Lancet 389:1741–1755
Levine JS, Burakoff R (2011) extraintestinal manifestations of inflammatory bowel disease. Gastroenterol Hepatol (NY) 7:235–241
Isaacs KL (2008) How prevalent are extra-intestinal manifestations at the initial diagnosis of IBD? Inflamm Bowel Dis 14:198–199
Wilson PWF (2008) Evidence of systemic inflammation and estimation of coronary artery disease risk: a population perspective. Am J Med 121:15–20
Dağlı N, Poyrazoğlu OK, Dağlı AF et al (2010) Is inflammatory bowel disease a risk factor for early atherosclerosis? Angiology 61:198–204
Isaacs KL, Lewis JD, Sandborn WJ et al (2005) State of the art: IBD therapy and clinical trials in IBD. Inflamm Bowel Dis 11:3–12
Pai JK, Pischon T, Ma J et al (2004) Inflammatory markers and the risk of coronary heart disease in men and women. N Engl J Med 351:2599–2610
Greenstein AJ, Sachar DB, Panday AK et al (1992) Amyloidosis and inflammatory bowel disease: a 50-year experience with 25 patients. Medicine Baltimore 71:261–270
Wester AL, Vatn MH, Fausa O (2001) Secondary amyloidosis in inflammatory bowel disease: a study of 18 patients admitted to Rikshospitalet University Hospital, Oslo, from 1962 to 1998. Inflamm Bowel Dis 7:295–300
Sarrouj BJ, Zampino DJ, Cilursu AM (1994) Pericarditis as the initial manifestation of inflammatory bowel disease. Chest 106:1911–1912
Sørensen HT, Fonager KM (1997) Myocarditis and inflammatory bowel disease a 16-year danish nationwide cohort study. Dan Med Bull 44:442–444
Li Z, Qiao L, Yun X et al (2021) Increased risk of ischemic heart disease and diabetes in inflammatory bowel disease. Z Gastroenterol 59:117–124
Gerche AL, Claessen G, Van de Bruaene A et al (2013) Cardiac MRI: a new gold standard for ventricular volume quantification during high-intensity exercise. Circ Cardiovasc Imaging 6:329–338
Xu RY, Zhu XF, Yang Y, Ye P (2013) High-sensitive cardiac troponin T. J Geriatr Cardiol 10:102–109
León D, Martín M, Corros C et al (2011) Usefulness of cardiac MRI in the early diagnosis of endomyocardial fibrosis. Rev Port Cardiol 31:401–402
Lichtenstein GR, Loftus EV, Isaacs KL et al (2018) ACG clinical guideline: management of Crohn’s disease in adults. Am J Gastroenterol 113:481–517
Fratz S, Chung T, Greil GF et al (2013) Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson 15:51
von Knobelsdorff-Brenkenhoff F, Schüler J, Dogangüzel S et al (2017) Detection and monitoring of acute myocarditis applying quantitative cardiovascular magnetic resonance. Circ Cardiovasc Imaging 10:e005242
Messroghli DR, Radjenovic A, Kozerke S et al (2004) Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med 52:141–146
Sprinkart AM, Luetkens JA, Träber F et al (2015) Gradient Spin Echo (GraSE) imaging for fast myocardial T2 mapping. J Cardiovasc Magn Reson 17:12
Cerqueira MD, Weissman NJ, Dilsizian V et al (2002) Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 105:539–542
Feng W, Chen G, Cai D et al (2017) Inflammatory bowel disease and risk of ischemic heart disease: an updated meta-analysis of cohort studies. J Am Heart Assoc 6:e005892
Runge C, Basit S, Ranthe MF et al (2013) Risk of ischaemic heart disease in patients with inflammatory bowel disease: a nationwide Danish cohort study. Gut 62:689–694
Bracamonte-Baran W, Čiháková D (2017) Cardiac autoimmunity: myocarditis. Adv Exp Med Biol 1003:187–221
Caforio ALP, Pankuweit S, Arbustini E et al (2013) Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 34:2636–2648
Friedrich MG, Sechtem U, Schulz-Menger J et al (2009) Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 53:1475–1487
Abdel-Aty H, Boye P, Zagrosek A et al (2005) Diagnostic performance of cardiovascular magnetic resonance in patients with suspected acute myocarditis: comparison of different approaches. J Am Coll Cardiol 45:1815–1822
Aarestrup J, Jess T, Kobylecki CJ et al (2019) Cardiovascular risk profile among patients with inflammatory bowel disease: a population-based study of more than 100 000 individuals. J Crohns Colitis 13:319–323
Kivrak T, Sunbul M, Cincin A et al (2016) Two-dimensional speckle tracking echocardiography is useful in early detection of left ventricular impairment in patients with Crohn’s disease. Eur Rev Med Pharmacol Sci 20:3249–3254
Hensel OK, Schneyder FEA, Wilke L et al (2017) Speckle tracking stress echocardiography uncovers early subclinical cardiac involvement in pediatric patients with inflammatory bowel diseases. Sci Rep 7:2966
Asadi J, Bhandari S, Ahmed N (2017) Mesalazine-induced myopericarditis in a patient with ulcerative colitis. Echo Research and Practice 5:K1–K5
Fontana M, Ćorović A, Scully P, Moon JC (2019) Myocardial amyloidosis: the exemplar interstitial disease. J Am Coll Cardiol Cardiovasc Imaging 12:2345–2356
Acknowledgements
The authors would like to thank Melahat Kırımlı (Philips healthcare, Turkey) for assistance in analyzing cardiac MR images.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
The Institutional Review Board statement.
The Institutional Review Board authorization agreement was given to conduct this research at and gather data from Pamukkale University Hospital.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
•Patients with Crohn’s disease (CD) had a higher myocardial ECV, mildly decreased RV-EF, and prolonged mean T2-relaxation time than healthy participants. There was an excellent agreement between observers for mean native T1, contrast enhanced T1-relaxation time, and mean T2-relaxation time measurements.
•Histogram analysis of T1/T2-mapping images demonstrated the maximum and mean T2-relaxation times were found to be higher in patients with CD, and mean T2-time was significantly correlated with ESR values in the measurements made by both observers with different software.
•The present study results suggest visually undetectable myocardial involvement due to systemic inflammation in patients with CD.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hasbey, I., Ufuk, F., Kaya, F. et al. Cardiac MRI findings in patients with Crohn’s disease. Ir J Med Sci 191, 1161–1169 (2022). https://doi.org/10.1007/s11845-021-02717-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-021-02717-w