
Abstract
Background
Hereditary haemochromatosis is often not diagnosed until adulthood. Iron overload cardiomyopathy initially results in diastolic dysfunction and can result in arrhythmias and irreversible cardiac failure if untreated. The aim of this study was to investigate whether patients with newly diagnosed hereditary haemochromatosis without signs of heart failure exhibit subclinical alterations of cardiac function and to determine if cardiac function improved after 1 year of venesection.
Methods
Baseline echocardiography was performed on 25 patients with newly diagnosed hereditary haemochromatosis with elevated serum ferritin levels. The test was repeated after 1 year of treatment with venesection. Tissue Doppler imaging (TDI) and deformation (strain) imaging using speckle tracking were performed. Left atrial force was measured according to the Newtonian principle, in which force (dynes) = mass × acceleration. Left atrial force was calculated by the Manning method expressed as ρ × 0.53 × mitral annular orifice area × (peak A velocity)2.
Results
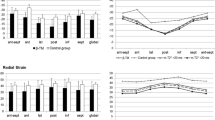
Radial strain showed a significant improvement after 1 year of venesection (increase from 38.8 to 52.6). The LAF showed a significant decrease after 1 year of venesection (median decrease = 0.6 (IQR 0, 1.60), p = 0.0004). Iso-volumetric relaxation time (IVRT) decreased significantly in patients after 1 year of venesection (decrease from 107.4 ± 16.2 to 97.68 ± 15.4 ms, p (0.0187)).
Conclusion
Among all measurements, radial strain, IVRT and left atrial force were shown to significantly improve following a 1-year course of venesection, suggesting that these parameters could be used to identify subclinical cardiac dysfunction in patients with iron overload secondary to hereditary haemochromatosis and to guide intensification of venesection therapy.


Similar content being viewed by others


References
Crownover BK, Covey CJ (2013) Hereditary hemochromatosis. Am Fam Physician 87(3):183–190
Carpenter JP, Grasso AE, Porter JB, Shah F, Dooley J, Pennell DJ (2013) On myocardial siderosis and left ventricular dysfunction in hemochromatosis. J Cardiovasc Magn Reson 15:24
Pietrangelo A (2003) Haemochromatosis. Gut 52(Suppl 2):ii23–ii30
Pietrangelo A (2015) Genetic, Genetic testing, and management of hemochromatosis: 15 years since hepcidin. Gastroenterology. 149(5):1240–51 e4
Tsushima RG, Wickenden AD, Bouchard RA, Oudit GY, Liu PP, Backx PH (1999) Modulation of iron uptake in heart by L-type Ca2+ channel modifiers: possible implications in iron overload. Circ Res 84(11):1302–1309
Horwitz LD, Rosenthal EA (1999) Iron-mediated cardiovascular injury. Vascular medicine (London, England) 4(2):93–99
Liu P, Olivieri N (1994) Iron overload cardiomyopathies: new insights into an old disease. Cardiovascular drugs and therapy / sponsored by the International Society of Cardiovascular Pharmacotherapy 8(1):101–110
Buja LM, Roberts WC (1971) Iron in the heart. Etiology and clinical significance. Am J Med 51(2):209–221
Fitchett DH, Coltart DJ, Littler WA, Leyland MJ, Trueman T, Gozzard DI et al (1980) Cardiac involvement in secondary haemochromatosis: a catheter biopsy study and analysis of myocardium. Cardiovasc Res 14(12):719–724
Shabanian R, Heidari-Bateni G, Kocharian A, Mashayekhi M, Hosseinzadeh S, Kiani A, Izadyar M, Koochakzadeh L (2010) Augmentation of left atrial contractile function: a herald of iron overload in patients with beta thalassemia major. Pediatr Cardiol 31(5):680–688
Seldrum S, Pierard S, Moniotte S, Vermeylen C, Vancraeynest D, Pasquet A, Vanoverschelde JL, Gerber BL (2011) Iron overload in polytransfused patients without heart failure is associated with subclinical alterations of systolic left ventricular function using cardiovascular magnetic resonance tagging. J Cardiovasc Magn Reson 13:23
Karamanou AG, Hamodraka ES, Vrakas SC, Paraskevaidis I, Lekakis I, Kremastinos DT (2014) Assessment of left ventricular and atrial diastolic function using two-dimensional (2D) strain imaging in patients with beta-thalassemia major. Eur J Haematol 92(1):59–65
Shizukuda Y, Bolan CD, Tripodi DJ, Yau YY, Nguyen TT, Botello G, Sachdev V, Sidenko S, Ernst I, Waclawiw MA, Leitman SF, Rosing DR (2006) Significance of left atrial contractile function in asymptomatic subjects with hereditary hemochromatosis. Am J Cardiol 98(7):954–959
Jahns R, Naito J, Tony HP, Inselmann G (1999) Atrial ejection force in systemic autoimmune diseases. Cardiology. 92(4):269–274
Kiani A, Kocharian A, Shabanian R, Rahimzadeh M, Shakibi JG (2008) Left atrial ejection force in healthy newborn infants. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 21(6):725–728
Manning WJ, Silverman DI, Katz SE, Douglas PS (1993) Atrial ejection force: a noninvasive assessment of atrial systolic function. J Am Coll Cardiol 22(1):221–225
Kremastinos DT, Farmakis D (2011) Iron overload cardiomyopathy in clinical practice. Circulation. 124(20):2253–2263
Carpenter JP, He T, Kirk P, Roughton M, Anderson LJ, de Noronha SV, Sheppard MN, Porter JB, Walker JM, Wood JC, Galanello R, Forni G, Catani G, Matta G, Fucharoen S, Fleming A, House MJ, Black G, Firmin DN, St. Pierre TG, Pennell DJ (2011) On T2* magnetic resonance and cardiac iron. Circulation. 123(14):1519–1528
Leonardi B, Margossian R, Colan SD, Powell AJ (2008) Relationship of magnetic resonance imaging estimation of myocardial iron to left ventricular systolic and diastolic function in thalassemia. J Am Coll Cardiol Img 1(5):572–578
[Available from: http://alcoholireland.ie/alcohol-and-you/guidelines/
EASL clinical practice guidelines for HFE hemochromatosis (2010) J Hepatol 53(1):3–22
Bacon BR, Adams PC, Kowdley KV, Powell LW, Tavill AS (2011) Diagnosis and management of hemochromatosis: 2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology (Baltimore, Md) 54(1):328–343
Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A (2009) Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 22(2):107–133
Yingchoncharoen T, Agarwal S, Popovic ZB, Marwick TH (2013) Normal ranges of left ventricular strain: a meta-analysis. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography 26(2):185–191
Olson LJ, Edwards WD, McCall JT, Ilstrup DM, Gersh BJ (1987) Cardiac iron deposition in idiopathic hemochromatosis: histologic and analytic assessment of 14 hearts from autopsy. J Am Coll Cardiol 10(6):1239–1243
Palka P, Macdonald G, Lange A, Burstow DJ (2002) The role of Doppler left ventricular filling indexes and Doppler tissue echocardiography in the assessment of cardiac involvement in hereditary hemochromatosis. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 15(9):884–890
Stanton T, Marwick TH (2010) Assessment of subendocardial structure and function. J Am Coll Cardiol Img 3(8):867–875
Kell DB (2009) Iron behaving badly: inappropriate iron chelation as a major contributor to the aetiology of vascular and other progressive inflammatory and degenerative diseases. BMC Med Genet 2:2
van Bokhoven MA, van Deursen CT, Swinkels DW (2011) Diagnosis and management of hereditary haemochromatosis. BMJ (Clinical research ed) 342:c7251
Oudit GY, Trivieri MG, Khaper N, Liu PP, Backx PH (2006) Role of L-type Ca2+ channels in iron transport and iron-overload cardiomyopathy. J Mol Med (Berlin, Germany) 84(5):349–364
Chen FE, Ooi C, Ha SY, Cheung BM, Todd D, Liang R et al (2000) Genetic and clinical features of hemoglobin H disease in Chinese patients. N Engl J Med 343(8):544–550
Kremastinos DT, Tsiapras DP, Tsetsos GA, Rentoukas EI, Vretou HP, Toutouzas PK (1993) Left ventricular diastolic Doppler characteristics in beta-thalassemia major. Circulation. 88(3):1127–1135
Ashley EA, Niebauer J (2004) Cardiology explained. Remedica, London
Acknowledgments
We would like to acknowledge and sincerely thank Ms. Liz Ellis who was the clinical nurse specialist for venesection treatment in St James Hospital at the time of our study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The Local Research Ethics Committee approved the study. Informed consent was obtained from each patient. Standard views and techniques were used according to the American Society of Echocardiography (ASE)/European Association of Echocardiography (EAE) guidelines.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Glossary
- ASE
-
American Society of Echocardiography
- UIBC
-
unsaturated iron binding capacity
- BSA
-
body surface area
- EAE
-
European Association of Echocardiography
- Fe
-
ferritin
- Hb
-
haemoglobin
- HH
-
hereditary haemochromatosis
- IVRT
-
iso-volumetric relaxation time
- LAF
-
left atrial force
- LAV max
-
left atrial volume
- LV
-
left ventricular
- MRI
-
magnetic resonance imaging
- STE
-
speckle tracking echocardiography
- TEI
-
myocardial performance index
- TIBC
-
total iron binding capacity
Rights and permissions
About this article

Cite this article
Byrne, D., Walsh, J.P., Daly, C. et al. Improvements in cardiac function detected using echocardiography in patients with hereditary haemochromatosis. Ir J Med Sci 189, 109–117 (2020). https://doi.org/10.1007/s11845-019-02032-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-019-02032-5