
Abstract
Background
Basic competency in musculoskeletal medicine is essential for many specialties being particularly relevant to primary care.
Aim
The purpose of this study was to objectively assess the adequacy of musculoskeletal education at multiple levels of medical training from undergraduate level to primary care.
Methods
A previously validated musculoskeletal examination was administered to 303 volunteers consisting of medical students, orthopaedic specialist registrars, general practice trainees and general practitioners.
Results
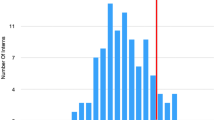
Forty (71%) general practitioners and 74 (71.8%) general practice trainees failed to obtain the passing score of 70. Sixty-three (87.5%) medical students who had completed an intensive 1-week long course in musculoskeletal medicine failed the examination. The pass rate improved significantly for general practitioners who had completed a postgraduate rotation in musculoskeletal medicine (47.8 vs 18.1%, P < 0.01).
Conclusions
These findings suggest that training in musculoskeletal medicine is inadequate at multiple levels of medical education with reform urgently required.



Similar content being viewed by others
References
Weinstein SL (2000) 2000–2010: the bone and joint decade. J Bone Joint Surg Am 82(1):1–3
Woolf AD, Akesson K (2001) Understanding the burden of musculoskeletal conditions. The burden is huge and not reflected in national health priorities. BMJ 322(7294):1079–1080
Simon LS (1999) Osteoarthritis: a review. Clin Cornerstone 2(2):26–37
Geyman JP, Gordon MJ (1979) Orthopedic problems in family practice: incidence, distribution, and curricular implications. J Fam Pract 8(4):759–765
Kahl LE (1987) Musculoskeletal problems in the family practice setting: guidelines for curriculum design. J Rheumatol 14(4):811–814
Marsland DW, Wood M, Mayo F (1976) Content of family practice. Part I. Rank order of diagnoses by frequency. Part II. Diagnoses by disease category and age/sex distribution. J Fam Pract 3(1):37–68
Mulhall KJ, Masterson E (2005) Relating undergraduate musculoskeletal medicine curricula to the needs of modern practice. Ir J Med Sci 174(2):46–51
Lynch JR, Gardner GC, Parsons RR (2005) Musculoskeletal workload versus musculoskeletal clinical confidence among primary care physicians in rural practice. Am J Orthop 34(10):487–491 (discussion)
Matzkin E, Smith EL, Freccero D, Richardson AB (2005) Adequacy of education in musculoskeletal medicine. J Bone Joint Surg Am 87(2):310–314
Matheny JM, Brinker MR, Elliott MN, Blake R, Rowane MP (2000) Confidence of graduating family practice residents in their management of musculoskeletal conditions. Am J Orthop 29(12):945–952
Sneiderman C (1977) Orthopedic practice and training of family physicians: a survey of 302 North Carolina practitioners. J Fam Pract 4(2):267–50
Clawson DK, Jackson DW, Ostergaard DJ (2001) It’s past time to reform the musculoskeletal curriculum. Acad Med 76(7):709–710
Freedman KB, Bernstein J (1998) The adequacy of medical school education in musculoskeletal medicine. J Bone Joint Surg Am 80(10):1421–1427
Freedman KB, Bernstein J (2002) Educational deficiencies in musculoskeletal medicine. J Bone Joint Surg Am 84-A(4):604–608
Lynch JR, Schmale GA, Schaad DC, Leopold SS (2006) Important demographic variables impact the musculoskeletal knowledge and confidence of academic primary care physicians. J Bone Joint Surg Am 88(7):1589–1595
Fowler PJ, Regan WD (1987) The patient with symptomatic chronic anterior cruciate ligament insufficiency. Results of minimal arthroscopic surgery and rehabilitation. Am J Sports Med 15(4):321–325
Booth A, Wise DI (1990) General practice training in musculoskeletal disorders. Br J Gen Pract 40(338):390
Pinney SJ, Regan WD (2001) Educating medical students about musculoskeletal problems. Are community needs reflected in the curricula of Canadian medical schools? J Bone Joint Surg Am 83-A(9):1317–1320
DiCaprio MR, Covey A, Bernstein J (2003) Curricular requirements for musculoskeletal medicine in American medical schools. J Bone Joint Surg Am 85-A(3):565–567
Williams JR (2000) The teaching of trauma and orthopaedic surgery to the undergraduate in the United Kingdom. J Bone Joint Surg Br 82(5):627–628
Conflict of interest
No financial support was sought for this study.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1
-
1.
What common problem must all newborns be examined for?
-
2.
What is a compartment syndrome?
-
3.
Acute septic arthritis of the knee may be differentiated from inflammatory arthritis by which laboratory test?
-
4.
A patient dislocates his knee in a car accident. What structure(s) is/are at risk for injury and therefore must be evaluated?
-
5.
A patient punches his companion in the face and sustains a fracture of the 5th metacarpal and a 3 mm break in the skin over the fracture. What is the correct treatment and why?
-
6.
A patient comes to the office complaining of low-back pain that wakes him from sleep. What two diagnoses are you concerned about?
-
7.
How is compartment syndrome treated?
-
8.
A patient lands on his hand and is tender to palpation in the “snuff box” (the space between the thumb extensor and abductor tendons). Initial radiographs do not show a fracture. What diagnosis must be considered?
-
9.
A 25-year old male is involved in a motor-vehicle accident. His left lower limb is in a position of flexion at the knee and hip, with internal rotation and adduction of the hip. What is the most likely diagnosis?
-
10.
What nerve is compressed in carpal tunnel syndrome?
-
11.
A patient has a disc herniation pressing on the 5th lumbar nerve root. How is motor function of the 5th lumbar nerve root tested?
-
12.
How is motor function of the median nerve tested in the hand?
-
13.
A 12-year-old-boy severely twists his ankle. Radiographs show only soft-tissue swelling. He is tender at the distal aspect of the fibula. What are the two possible diagnoses?
-
14.
A patient presents with new-onset low back pain. Under what conditions are plain radiographs indicated? Please name five (example history of trauma).
-
15.
A patient has a displaced fracture near the fibular neck. What structure is at risk for injury?
-
16.
A 20-year-old injured his knee while playing football. You see him on the same day, and he has a knee effusion. An aspiration shows frank blood. What are the three most common diagnoses?
-
17.
What are the five most common sources of cancer metastatses to bone?
-
18.
Name two differences between rheumatoid arthritis and osteoarthritis.
-
19.
What malignancy may be present in bone yet typically is not detected with a bone scan?
-
20.
What is the function of the normal anterior cruciate ligament at the knee?
-
21.
What is the difference between osteoporosis and osteomalacia?
-
22.
In elderly patients, displaced fractures of the femoral neck are typically treated with joint replacement, whereas fractures near the trochanter are treated with plates and screws. Why?
-
23.
What muscle(s) is/are involved in lateral epicondylitis (tennis elbow)?
-
24.
Rupture of the biceps at the elbow results in weakness of both elbow flexion and ___________?
-
25.
What muscle(s) control(s) external rotation of the humerus with the arm at the side?
Appendix 2

Rights and permissions
About this article
Cite this article
Queally, J.M., Kiely, P.D., Shelly, M.J. et al. Deficiencies in the education of musculoskeletal medicine in Ireland. Ir J Med Sci 177, 99–105 (2008). https://doi.org/10.1007/s11845-008-0153-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-008-0153-z