
Abstract
Objectives
To investigate the incidence of and the risk factors for early postoperative pulmonary complications (PPC) after minimally invasive esophagectomy (MIE) in the prone position from the perspective of anesthetic management.
Methods
We conducted a historical cohort study of patients who underwent MIE in the prone position between September 2010 and August 2018. PPC was defined as pneumonia, atelectasis, acute respiratory distress syndrome (ARDS), respiratory failure, and pulmonary embolism (Clavien–Dindo Classification Grade II or higher) that occurred within 7 days after MIE.
Results
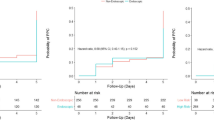
Out of 489 patients, there were 90 patients (18.4%) with PPC: 75 patients with pneumonia, 24 patients with atelectasis, 13 patients with respiratory failure, 6 patients with ARDS, and 2 patients with pulmonary embolism. Twenty-eight patients suffered from 2 or more components of PPC. PPC patients were older (66.6 vs. 63.6 year, P = 0.038) and had higher amount of crystalloid (4200 vs. 3550 mL, P < 0.0001), and longer duration of anesthesia (670 vs. 625 min, P = 0.0062) than non-PPC patients. PPC patients were more likely to have had chronic obstructive pulmonary disease (COPD) (26.7 vs. 7.8%, P < 0.001). Incidence of PPC was significantly higher in patients with one-lung ventilation than with two-lung ventilation (37.1 vs. 15.3%, P < 0.001). Multivariable logistic regression analysis showed that PPC was associated with age (per 10 years, odds ratio (OR) = 1.41), COPD (OR = 3.43), one-lung ventilation (OR = 1.94), and volume of crystalloid (per 500 mL, OR = 1.22).
Conclusions
Two-lung rather than one-lung ventilation should be chosen and fluid overload should be avoided in patients undergoing MIE in the prone position.

Similar content being viewed by others


References
Oshikiri T, Takiguchi G, Miura S, Takase N, Hasegawa H, Yamamoto M, et al. Current status of minimally invasive esophagectomy for esophageal cancer: is it truly less invasive? Ann Gastroenterol Surg. 2018;3:138–45.
Cuesta MA, van der Wielen N, Straatman J, van der Peet DL. Video-assisted thoracoscopic esophagectomy: keynote lecture. Gen Thorac Cardiovasc Surg. 2016;64:380–5.
Cuschieri A. Thoracoscopic subtotal oesophagectomy. Endosc Surg Allied Technol. 1994;2:21–5.
Saikawa D, Okushiba S, Kawata M, Okubo T, Kitashiro S, Kawarada Y, et al. Efficacy and safety of artificial pneumothorax under two-lung ventilation in thoracoscopic esophagectomy for esophageal cancer in the prone position. Gen Thorac Cardiovasc Surg. 2014;62:163–70.
Michelet P, D’Journo XB, Roch A, Doddoli C, Marin V, Papazian L, et al. Protective ventilation influences systemic inflammation after esophagectomy: a randomized controlled study. Anesthesiology. 2006;105:911–9.
Biere SS, van Berge Henegouwen MI, Maas KW, Bonavina L, Rosman C, Garcia JR, et al. Minimally invasive versus open oesophagectomy for patients with oesophaeal cancer: a multicentre, open-label, randomized controlled trial. Lancet. 2012;379:1887–92.
Kanekiyo S, Takeda S, Tsutsui M, Nishiyama M, Kitahara M, Shindo Y, et al. Low invasiveness of thoracoscopic esophagectomy in the prone position for esophageal cancer: a propensity score-matched comparison of operative approaches between thoracoscopic and open esophagectomy. Surg Endosc. 2018;32:1945–53.
Molena D, Mungo B, Stem M, Lidor AO. Incidence and risk factors for respiratory complications in patients undergoing esophagectomy for malignancy: a NSQIP analysis. Semin Thorac Cardiovasc Surg. 2014;26:287–94.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147:573–7.
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187–96.
Zingg U, Smithers BM, Gotley DC, Smith G, Aly A, Clough A, et al. Factors associated with postoperative pulmonary morbidity after esophagectomy for cancer. Ann Surg Oncol. 2011;18:1460–8.
Yoshida N, Baba Y, Hiyoshi Y, Shigaki H, Kurashige J, Sakamoto Y, et al. Duration of smoking cessation and postoperative morbidity after esophagectomy for esophageal cancer: how long should patients stop smoking before surgery? World J Surg. 2016;40:142–7.
Shen Y, Zhong M, Wu W, et al. The impact of tidal volume on pulmonary complications following minimally invasive esophagectomy: a randomized and controlled study. J Thorac Cardiovasc Surg. 2013;146:1267–74.
Casado D, Lopez F, Marti R. Perioperative fluid management and major respiratory complications in patients undergoing esophagectomy. Dis Esophagus. 2010;23:523–8.
Weijs TJ, Ruurda JP, Nieuwenhuijzen GAP, van Hillegersberg R, Luyer MDP. Strategies to reduce pulmonary complications after esophagectomy. World J Gastroenterol. 2013;19:6509–14.
Funding
This work was funded by the Department of Anesthesiology, The Cancer Institute Hospital of Japanese Foundation for Cancer Research, Japan.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest associated with this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ishikawa, S., Ozato, S., Ebina, T. et al. Early postoperative pulmonary complications after minimally invasive esophagectomy in the prone position: incidence and perioperative risk factors from the perspective of anesthetic management. Gen Thorac Cardiovasc Surg 70, 659–667 (2022). https://doi.org/10.1007/s11748-022-01818-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-022-01818-2