
Abstract
Objectives
Aortic surgeries performed under moderate hypothermia require antegrade cerebral perfusion. The influence of retrograde cerebral perfusion under moderate hypothermic circulatory arrest remains unknown. To clarify this effect, this study aimed to compare the early outcomes of retrograde versus antegrade cerebral perfusion under moderate hypothermia for hemiarch replacement.
Methods
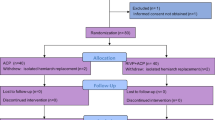
Between March 2009 and April 2020, 391 hemiarch replacements under moderate hypothermic circulatory arrest via median sternotomy were performed at our institution. Of these, 70 involved retrograde perfusion and 162 involved antegrade perfusion. Propensity score matching was used to compare 61 pairs of retrograde and antegrade cases.
Results
Retrograde and antegrade strategy under moderate hypothermia resulted in comparable operative mortality (3.3% vs. 1.6%, P > 0.99), permanent neurological deficits (8.5% vs. 6.6%, P > 0.99), and temporary neurological deficits (24.6% vs. 39.3%, P = 0.33). Retrograde surgery was associated with shorter circulatory arrest times (31.4 ± 8.2 min vs. 37.4 ± 12.2 min, P = 0.005) and fewer red blood cell transfusions (4.6 ± 3.9 units vs. 8.2 ± 5.1 units, P < 0.001) than those with antegrade surgery.
Conclusions
Retrograde cerebral perfusion under moderate hypothermia for hemiarch replacement yields excellent operative outcomes, equivalent to those achieved using an antegrade strategy.

Similar content being viewed by others


References
Fan S, Li H, Wang D, Wu C, Pan Z, Li Y, et al. Effects of four major brain protection strategies during proximal aortic T surgery: a systematic review and network meta-analysis. Int J Surg. 2019;63:8–15.
Milewski RK, Pacini D, Moser GW, Moeller P, Cowie D, Szeto WY, et al. Retrograde and antegrade cerebral perfusion: results in short elective arch reconstructive times. Ann Thorac Surg. 2010;89:1448–57.
Okita Y, Minatoya K, Tagusari O, Ando M, Nagatsuka K, Kitamura S. Prospective comparative study of brain protection in total aortic arch replacement: deep hypothermic circulatory arrest with retro-grade cerebral perfusion or selective antegrade cerebral perfusion. Ann Thorac Surg. 2001;72:72–9.
Okita Y, Okada K, Omura A, Kano H, Minami H, Inoue T, et al. Total arch replacement using selective antegrade cerebral perfusion as the neuroprotection strategy. Ann Cardiothorac Surg. 2013;2:169–74.
Ganapathi AM, Hanna JM, Schechter MA, Englum BR, Castleberry AW, Gaca JG, et al. Antegrade versus retrograde cerebral perfusion for hemiarch replacement with deep hypothermic circulatory arrest: does it matter? A propensity-matched analysis. J Thorac Cardiovasc Surg. 2014;148:2896–902.
De Paulis R, Czerny M, Weltert L, Bavaria J, Borger MA, Carrel TP, et al. Current trends in cannulation and neuroprotection during surgery of the aortic arch in Europe. Eur J Cardiothorac Surg. 2015;47:917–23.
Englum BR, He X, Gulack BC, Ganapathi AM, Mathew JP, Brennan JM, et al. Hypothermia and cerebral protection strategies in aortic arch surgery: a comparative effectiveness analysis from the STS Adult Cardiac Surgery Database. Eur J Cardiothorac Surg. 2017;52:492–8.
Ueda Y, Miki S, Kusuhara K, Okita Y, Tahata T, Yamanaka K. Surgical treatment of aneurysm or dissection involving the ascending aorta and aortic arch, utilising circulatory arrest and retrograde cerebral perfusion. J Cardiovasc Surg (Torino). 1990;31:553–8.
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48:452–8.
Moshkovitz Y, David TE, Caleb M, Feindel CM, de Sa MP. Circulatory arrest under moderate systemic hypothermia and cold retrograde cerebral perfusion. Ann Thorac Surg. 1998;66:1179–83.
Tokuda Y, Miyata H, Motomura N, Oshima H, Usui A, Takamoto S, et al. Brain protection during ascending aortic repair for Stanford type A acute aortic dissection surgery. Nationwide analysis in Japan. Circ J. 2014;78:2431–8.
Ueda T, Shimizu H, Ito T, Kashima I, Hashizume K, Iino Y, et al. Cerebral complications associated with selective perfusion of the arch vessels. Ann Thorac Surg. 2000;70:1472–7.
Antilla V, Pokela M, Kiviluoma K, Mäkiranta M, Hirvonen J, Juvonen T. Is maintained cranial hypothermia the only factor leading to improved outcome after retrograde cerebral perfusion? An experimental study with a chronic porcine model. J Thorac Cardiovasc Surg. 2000;119:1021–9.
Juvonen T, Weisz DJ, Wolfe D, Zhang N, Bodian CA, McCullough JN, et al. Can retrograde perfusion mitigate cerebral injury after particulate embolisation? A study in a chronic porcine model. J Thorac Cardiovasc Surg. 1998;115:1142–59.
Ghoreishi M, Sundt TM, Cameron DE, Holmes SD, Roselli EE, Pasrija C, et al. Factors associated with acute stroke after type A aortic dissection repair: an analysis of the Society of Thoracic Surgeons National Adult Cardiac Surgery Database. J Thorac Cardiovasc Surg. 2020;159:2143–54.
Leshnower BG, Rangaraju S, Allen JW, Stringer AY, Gleason TG, Chen EP. Deep hypothermia with retrograde cerebral perfusion versus moderate hypothermia with antegrade cerebral perfusion for arch surgery. Ann Thorac Surg. 2019;107:1104–10.
Williams JB, Peterson ED, Zhao Y, O’Brien SM, Andersen ND, Miller DC, et al. Contemporary results for proximal aortic replacement in North America. J Am Coll Cardiol. 2012;60:1156–62.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Authors have no conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nakahara, Y., Tsukioka, Y., Tateishi, R. et al. Safety of retrograde cerebral perfusion under moderate hypothermia for hemiarch replacement. Gen Thorac Cardiovasc Surg 70, 842–849 (2022). https://doi.org/10.1007/s11748-022-01814-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-022-01814-6